

Review
doi: 10.1136/hrt.2003.019927.
Theory and practice of defibrillation: (2) defibrillation for ventricular fibrillation
Affiliations
- PMID: 15604356
- PMCID: PMC1768652
- DOI: 10.1136/hrt.2003.019927
Item in Clipboard
Review
Theory and practice of defibrillation: (2) defibrillation for ventricular fibrillation
Heart.
2005 Jan.
No abstract available
Figures
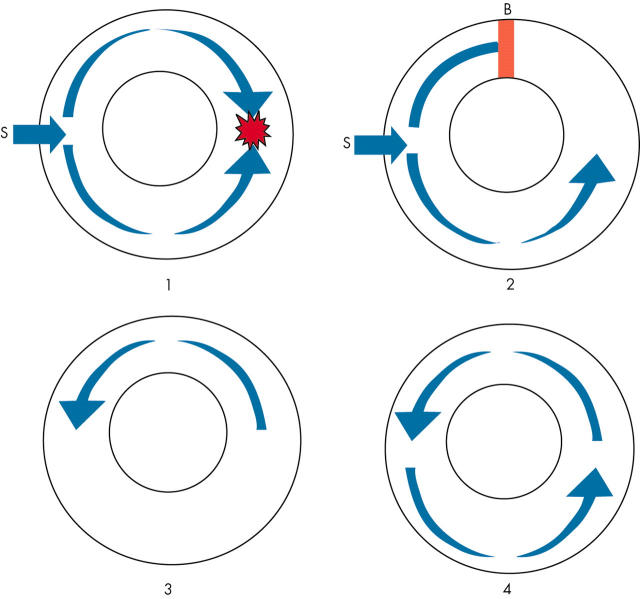
Re-entry. In normal tissue (panel 1) an electrical stimulus (S) will produce wavefronts that travel in both directions. These will collide and die out. In panel 2, an area of conduction block is present (B). The upper wavefront produced by the stimulus (S) dies out as it encounters the area of block. However, the lower wavefront continues to travel around the tissue. By the time this wavefront reaches the upper half of the ring of cardiac tissue, the conduction block has resolved and a re-entrant wavefront is established (panels 3 and 4).
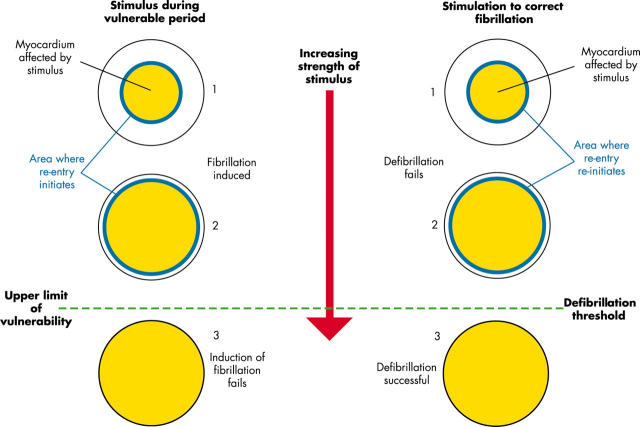
Relation between the upper limit of vulnerability and defibrillation threshold. The myocardium affected by the electrical stimulus is represented in yellow. In the left half of the diagram shocks are delivered to induce VF during the vulnerable period while in the right half of the diagram shocks are delivered during VF to attempt defibrillation. As the strength of electrical stimulus increases from 1 to 2, the area of myocardium affected increases. The zone where re-entry occurs after the shock (blue region) moves away from the area where the shock is delivered. A further increase in the intensity of stimulus (3) affects all of the myocardium and prevents induction of VF above the upper limit of vulnerability and successfully defibrillates above the defibrillation threshold.
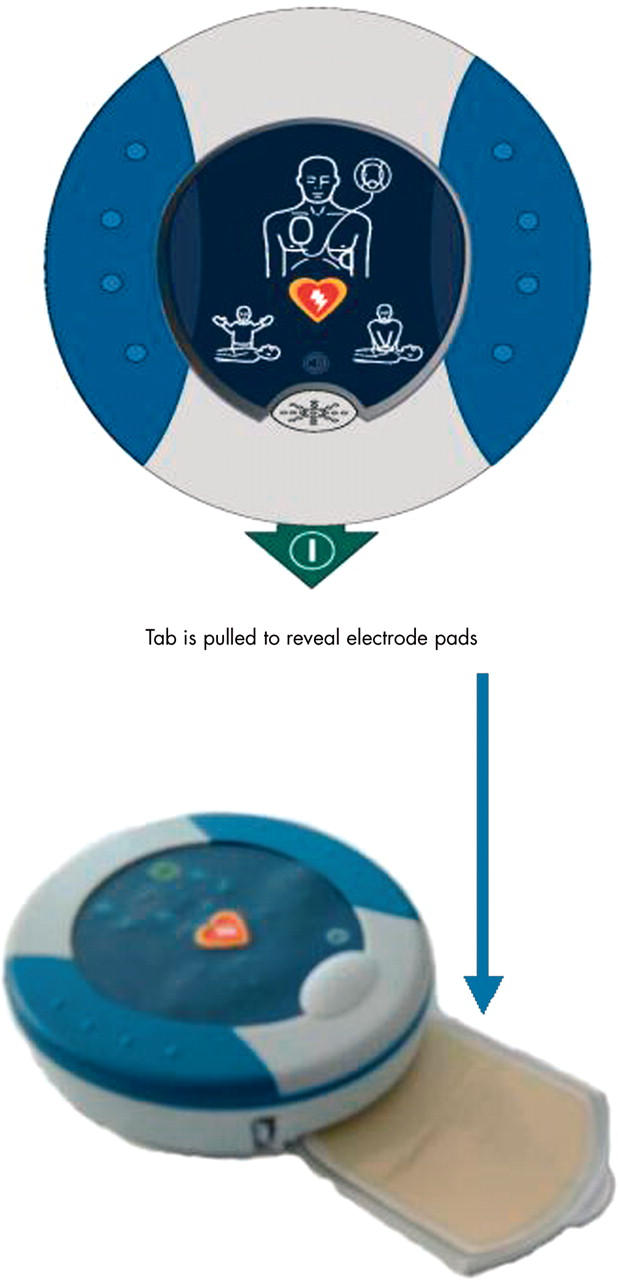
Automated external defibrillator (AED) intended for use by the general public (weight 1 kg).
References
-
- Ideker RE, Wolf PD, Tang ASL. Mechanisms of defibrillation. In: Tacker WA, ed. Defibrillation of the heart. St Louis, Missouri: Mosby-Year Book, Inc, 1994:15–45.
-
- Ideker RE, Chattipakorn N, Gray RA. Defibrillation mechanisms: the parable of the blind men and the elephant. J Cardiovasc Electrophysiol 2000;11:1008–13. Review of the mechanisms of defibrillation. - PubMed
-
- Dillon SM, Kwaku KF. Progressive depolarization. A unified hypothesis for defibrillation and fibrillation induction by shocks. J Cardiovasc Electrophysiol 1998;9:529–52. Thorough examination of theories of defibrillation. - PubMed
-
- ECC Guidelines. Part 6: Advanced cardiovascular life support: section 2: defibrillation. Circulation 2000;102 (suppl I) :I90–4. - PubMed
-
- Resuscitation Council (UK). Adult advanced life support. Resuscitation Guidelines 2000. http://www.resus.org.uk/pages/als.htm. Current UK Resuscitation Council Guidelines.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources