

Echocardiographic AV-interval optimization in patients with reduced left ventricular function
- PMID: 15606916
- PMCID: PMC544593
- DOI: 10.1186/1476-7120-2-30
Echocardiographic AV-interval optimization in patients with reduced left ventricular function
Abstract
Background: Ritter's method is a tool used to optimize AV delay in DDD pacemaker patients with normal left ventricular function only. The goal of our study was to evaluate Ritter's method in AV delay-interval optimization in patients with reduced left ventricular function.
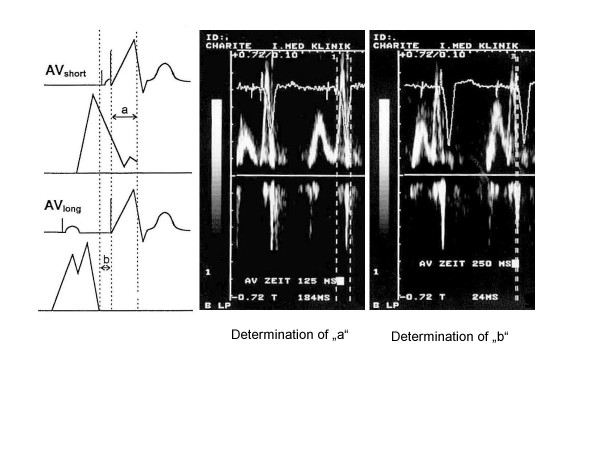
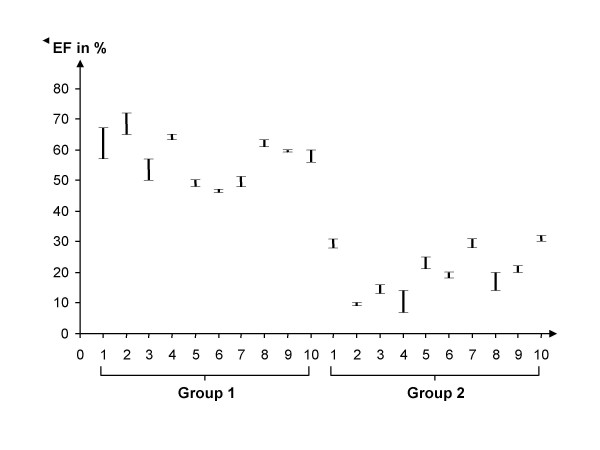
Methods: Patients with implanted DDD pacemakers and AVB III degrees were assigned to one of two groups according to ejection fraction (EF): Group 1 (EF > 35%) and Group 2 (EF < 35%). AV delay optimization was performed by means of radionuclide ventriculography (RNV) and application of Ritter's method.
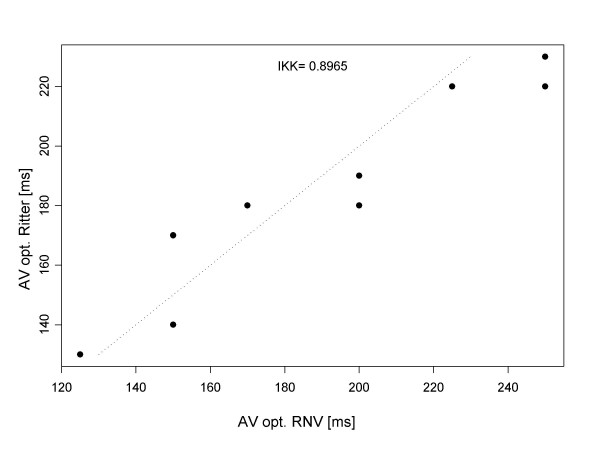
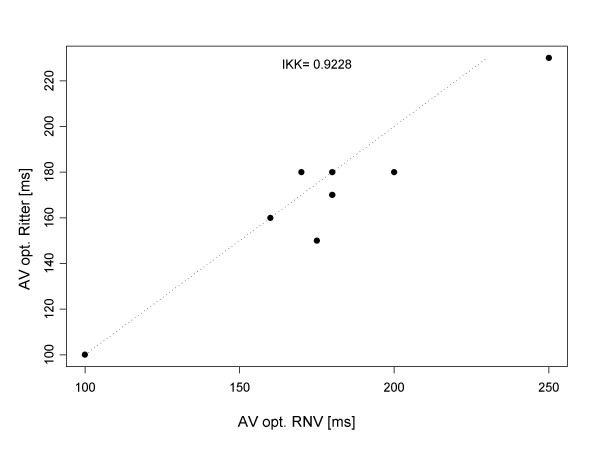
Results: For each of the patients examined, we succeeded in defining an optimal AV interval by means of both RNV and Ritter's method. The optimal AV delay determined by RNV correlated well with the delay found by Ritter's method, especially among those patients with reduced EF. The intra-class correlation coefficient was 0.8965 in Group 1 and 0.9228 in Group 2. The optimal AV interval in Group 1 was 190 +/- 28.5 ms, and 180 +/- 35 ms in Group 2.
Conclusion: Ritter's method is also effective for optimization of AV intervals among patients with reduced left ventricular function (EF < 35%). The results obtained by RNV correlate well with those from Ritter's method. Individual programming of the AV interval is fundamentally essential in all cases.
Figures
Similar articles
-
Utilization of Electrocardiographic P-wave Duration for AV Interval Optimization in Dual-Chamber Pacemakers.Indian Pacing Electrophysiol J. 2010 Sep 5;10(9):383-92. Indian Pacing Electrophysiol J. 2010. PMID: 20930956 Free PMC article.
-
Influence of the atrio-ventricular delay optimization on the intra left ventricular delay in Cardiac Resynchronization Therapy.Cardiovasc Ultrasound. 2006 Jan 26;4:5. doi: 10.1186/1476-7120-4-5. Cardiovasc Ultrasound. 2006. PMID: 16436217 Free PMC article. Clinical Trial.
-
Correlation of echo-Doppler optimization of atrioventricular delay in cardiac resynchronization therapy with invasive hemodynamics in patients with heart failure secondary to ischemic or idiopathic dilated cardiomyopathy.Am J Cardiol. 2006 Feb 15;97(4):552-7. doi: 10.1016/j.amjcard.2005.08.076. Epub 2006 Jan 4. Am J Cardiol. 2006. PMID: 16461055
-
Shorter AV delays provide improved echocardiographic hemodynamics during exercise in patients receiving cardiac resynchronization therapy.Pacing Clin Electrophysiol. 2009 Apr;32(4):457-65. doi: 10.1111/j.1540-8159.2009.02305.x. Pacing Clin Electrophysiol. 2009. PMID: 19335854 Clinical Trial.
-
Heart rate variability in patients suffering from structural heart disease and decreased AV-nodal conduction capacity. Insights into the formation of heart rate variability.Z Kardiol. 2004 Mar;93(3):229-33. doi: 10.1007/s00392-004-0050-z. Z Kardiol. 2004. PMID: 15024591
Cited by
-
Echocardiographic demonstration of the effect of varying paced a-v intervals on ventricular filling pattern.Indian Pacing Electrophysiol J. 2008 Aug 1;8(3):218-21. Indian Pacing Electrophysiol J. 2008. PMID: 18679522 Free PMC article. No abstract available.
-
Progress in Cardiac Resynchronisation Therapy and Optimisation.J Cardiovasc Dev Dis. 2023 Oct 17;10(10):428. doi: 10.3390/jcdd10100428. J Cardiovasc Dev Dis. 2023. PMID: 37887875 Free PMC article. Review.
-
Utilization of Electrocardiographic P-wave Duration for AV Interval Optimization in Dual-Chamber Pacemakers.Indian Pacing Electrophysiol J. 2010 Sep 5;10(9):383-92. Indian Pacing Electrophysiol J. 2010. PMID: 20930956 Free PMC article.
References
-
- Ausubel K, Klementowicz P, Furman S. Interatrial conduction during cardiac pacing. PACE. 1986;9:1026–1031. - PubMed
-
- Stierle U, Schmücker G, Potratz J. Das interatriale Leitungsverhalten bei AV-sequentieller Stimulation – eine elektrokardiographische Studie. Herzschr Elektrophys. 1992;3:101–109.
-
- Camous JP, Raybound F, Dolisi C, Schenowitz A, Varenne A, Baudouy M. Interatrial conduction in patients undergoing AV stimulation: effects of increasing right atrial stimulation rate. PACE. 1993;16:2082–2086. - PubMed
-
- Haskell RJ, French WJ. Optimum AV interval in dual chamber pacemakers. PACE. 1986;9:670–674. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
