

Utility of hemoglobin A1c in predicting diabetes risk
- PMID: 15610327
- PMCID: PMC1492588
- DOI: 10.1111/j.1525-1497.2004.40178.x
Utility of hemoglobin A1c in predicting diabetes risk
Abstract
Background: There is controversy surrounding the issue of whether, and how, to screen adults for type 2 diabetes. Our objective was to measure the incidence of new diabetes among outpatients enrolled in a health care system, and to determine whether hemoglobin A1c (HbA1c) values would allow risk stratification for patients' likelihood of developing diabetes over 3 years.
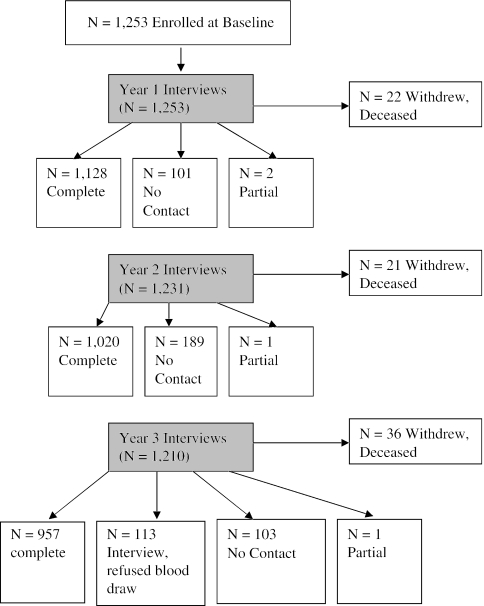
Methods: We conducted a prospective cohort study with 3-year follow-up at a single large, tertiary care, Department of Veterans Affairs Medical Center (VAMC). A convenience sample of 1,253 outpatients without diabetes, age 45 to 64, with a scheduled visit at the VAMC, were screened for diabetes using an initial HbA1c measurement. All subjects with HbA1c > or = 6.0% (normal, 4.0% to 6.0%) were invited for follow-up fasting plasma glucose (FPG). We then surveyed patients annually for 3 years to ascertain interval diagnosis of diabetes by a physician. The baseline screening process was repeated 3 years after initial screening. After the baseline screening, new cases of diabetes were defined as either the self-report of a physician's diagnosis of diabetes, or by HbA1c > or = 7.0% or FPG > or = 7.0 mmol/L at 3-year follow-up. The incidence of diabetes was calculated as the number of new cases per person-year of follow-up.
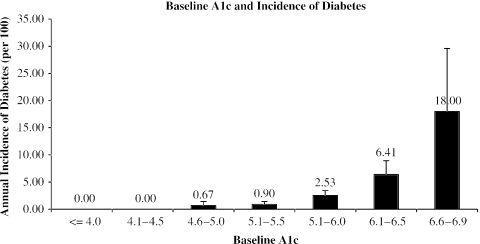
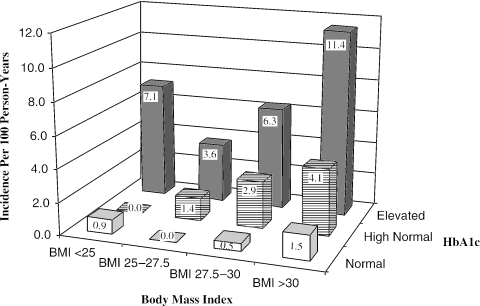
Results: One thousand two hundred fifty-three patients were screened initially, and 56 (4.5%) were found to have prevalent unrecognized diabetes at baseline. The 1,197 patients without diabetes at baseline accrued 3,257 person-years of follow-up. There were 73 new cases of diabetes over 3 years of follow-up, with an annual incidence of 2.2% (95% confidence interval [CI], 1.7% to 2.7%). In a multivariable logistic regression model, baseline HbA1c and baseline body mass index (BMI) were the only significant predictors of new onset diabetes, with HbA1c having a greater effect than BMI. The annual incidence of diabetes for patients with baseline HbA1c < or = 5.5 was 0.8% (CI, 0.4% to 1.2%); for HbA1c 5.6 to 6.0, 2.5% (CI, 1.6% to 3.5%); and for HbA1c 6.1 to 6.9, 7.8% (CI, 5.2% to 10.4%). Obese patients with HbA1c 5.6 to 6.0 had an annual incidence of diabetes of 4.1% (CI, 2.2% to 6.0%).
Conclusions: HbA1c testing helps predict the likelihood that patients will develop diabetes in the future. Patients with normal HbA1c have a low incidence of diabetes and may not require rescreening in 3 years. However, patients with elevated HbA1c who do not have diabetes may need more careful follow-up and possibly aggressive treatment to reduce the risk of diabetes. Patients with high-normal HbA1c may require follow-up sooner than 3 years, especially if they are significantly overweight or obese. This predictive value suggests that HbA1c may be a useful test for periodic diabetes screening.
Figures
References
-
- Harris MI. Noninsulin-dependent diabetes mellitus in black and white Americans. Diabetes Metab Rev. 1990;6:71–90. - PubMed
-
- Harris MI. Impaired glucose tolerance in the US population. Diabetes Care. 1989;12:464–74. - PubMed
-
- Huse DM, Oster G, Killen AR, Lacey MJ, Colditz GA. The economic costs of non-insulin-dependent diabetes mellitus. JAMA. 1989;262:2708–13. - PubMed
-
- Harris MI, Klein R, Welborn TA, Knuiman MW. Onset of NIDDM occurs at least 4–7 years before clinical diagnosis. Diabetes Care. 1992;15:815–9. - PubMed
-
- Anonymous. VA Diabetes Clinical Practice Guidelines. Available at: http://209.42.214.199/cpg/DM/DM_base.htm. Accessed October 11, 2004.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical