

Prevalence of the insulin resistance syndrome in obesity
- PMID: 15613503
- PMCID: PMC1720077
- DOI: 10.1136/adc.2003.036467
Prevalence of the insulin resistance syndrome in obesity
Abstract
Aims: To assess prevalence of the insulin resistance syndrome (IRS: obesity, abnormal glucose homoeostasis, dyslipidaemia, and hypertension) in obese UK children and adolescents of different ethnicities and to assess whether fasting data is sufficient to identify IRS in childhood obesity.
Methods: A total of 103 obese (BMI >95th centile) children and adolescents 2-18 years of age referred for assessment underwent an oral glucose tolerance test, measurement of fasting lipids, and blood pressure determination. Main outcome measures were prevalence of components of IRS by modified WHO criteria, with IRS defined as > or =3 components (including obesity).
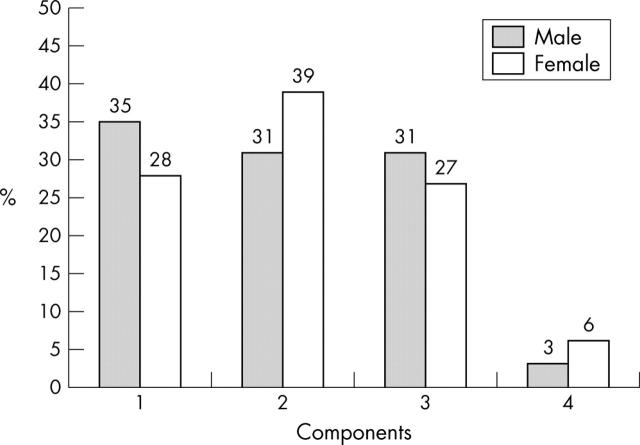
Results: There were 67 girls (65%). BMI z-score ranged from 1.65 to 6.15, with 72% having a z-score > or =3.0. Abnormal glucose homoeostasis was identified in 46% (hyperinsulinism in 40%, impaired fasting glucose in 0.8%, impaired glucose tolerance in 11%). No subjects had silent type 2 diabetes. Dyslipidaemia was identified in 30% and hypertension in 32%. Thirty one per cent had obesity alone, 36% had two components, 28% had three, and 5% had all four components. Birth weight, BMI, and family history of IRS were not associated with risk of IRS. Higher age increased the risk of IRS; however the syndrome was seen in 30% of children under 12 years. The use of fasting glucose and insulin data for identifying IRS had a sensitivity of 88% and specificity of 100%.
Conclusions: One third of obese children and adolescents have the IRS; however type 2 diabetes is rare. Obese children with the IRS may form a high risk group to whom scarce intervention resources should be targeted. Further work is needed to develop appropriate screening programmes for IRS components in significantly obese children.
Figures
Comment in
-
Obesity and the insulin resistance syndrome.Arch Dis Child. 2005 Jan;90(1):1. doi: 10.1136/adc.2003.046854. Arch Dis Child. 2005. PMID: 15613499 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical