

Nefopam and ketamine comparably enhance postoperative analgesia
- PMID: 15616073
- PMCID: PMC1283103
- DOI: 10.1213/01.ANE.0000138037.19757.ED
Nefopam and ketamine comparably enhance postoperative analgesia
Abstract
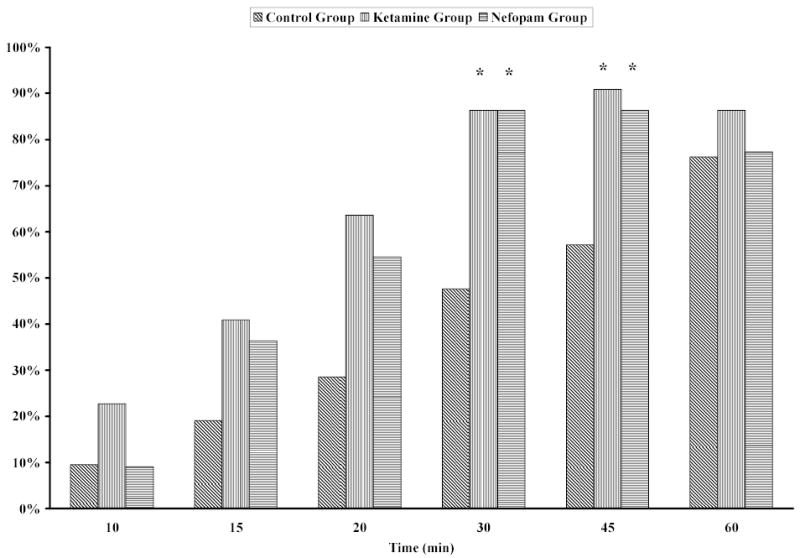
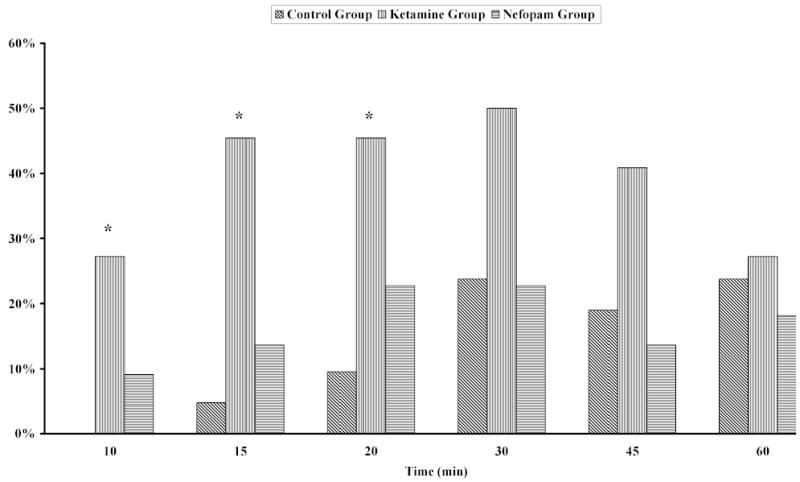
Opioids alone sometimes provide insufficient postoperative analgesia. Coadministration of drugs may reduce opioid use and improve opioid efficacy. We therefore tested the hypothesis that the administration of ketamine or nefopam to postoperative patients with pain only partly alleviated by morphine reduces the amount of subsequent opioid necessary to produce adequate analgesia. Patients (n=77) recovering from major surgery were given up to 9 mg of IV morphine. Those who still had pain were randomly assigned to blinded administration of 1) isotonic saline (control group; n=21), 2) ketamine 10 mg (ketamine group; n=22), or 3) nefopam 20 mg (nefopam group; n=22). Three-milligram morphine boluses were subsequently given at 5-min intervals until adequate analgesia was obtained, until 60 min elapsed after the beginning of study drug administration, or until ventilation became insufficient (respiratory rate <10 breaths/min or saturation by pulse oximetry <95%). Supplemental morphine (i.e., after test drug administration) requirements were significantly more in the control group (mean +/- sd; 17 +/- 10 mg) than in the nefopam (10 +/- 5 mg; P <0.005) or ketamine (9 +/- 5 mg; P <0.001) groups. Morphine titration was successful in all ketamine and nefopam patients but failed in four control patients (two because of respiratory toxicity and two because of persistent pain). Tachycardia and profuse sweating were more frequent in patients given nefopam, and sedation was more intense with ketamine; however, the incidence of other potential complications did not differ among groups.
Figures
References
-
- Paqueron X, Lumbroso A, Mergoni P, et al. Is morphine-induced sedation synonymous with analgesia during intravenous morphine titration? Br J Anaesth. 2002;89:697–701. - PubMed
-
- Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77:1048–56. - PubMed
-
- Kohrs R, Durieux ME. Ketamine: teaching an old drug new tricks. Anesth Analg. 1998;87:1186–93. - PubMed
-
- Schmid RL, Sandler AN, Katz J. Use and efficacy of low-dose ketamine in the management of acute postoperative pain: a review of current techniques and outcomes. Pain. 1999;82:111–25. - PubMed
-
- Menigaux C, Fletcher D, Dupont X, et al. The benefits of intraoperative small-dose ketamine on postoperative pain after anterior cruciate ligament repair. Anesth Analg. 2000;90:129–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
