

Surgeon specialty and operative mortality with lung resection
- PMID: 15622006
- PMCID: PMC1356861
- DOI: 10.1097/01.sla.0000149428.17238.03
Surgeon specialty and operative mortality with lung resection
Abstract
Objective: We sought to examine the effect of subspecialty training on operative mortality following lung resection.
Summary background data: While several different surgical subspecialists perform lung resection for cancer, many believe that this procedure is best performed by board-certified thoracic surgeons.
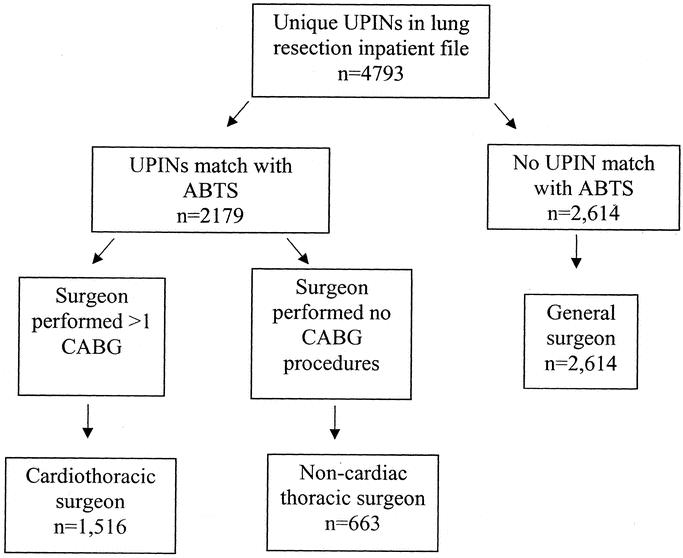
Methods: Using the national Medicare database 1998 to 1999, we identified patients undergoing lung resection (lobectomy or pneumonectomy) for lung cancer. Operating surgeons were identified by unique physician identifier codes contained in the discharge abstract. We used the American Board of Thoracic Surgery database, as well as physician practice patterns, to designate surgeons as general surgeons, cardiothoracic surgeons, or noncardiac thoracic surgeons. Using logistic regression models, we compared operative mortality across surgeon subspecialties, adjusting for patient, surgeon, and hospital characteristics.
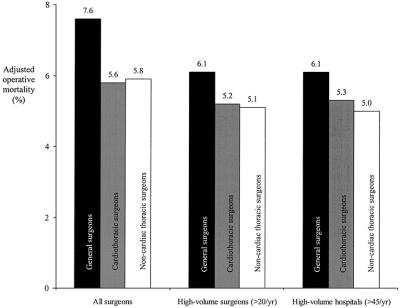
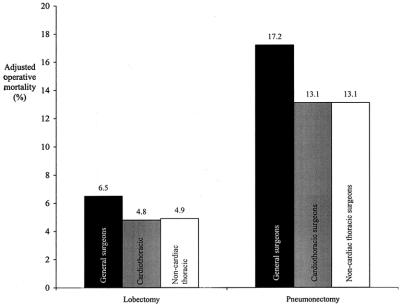
Results: Overall, 25,545 Medicare patients underwent lung resection, 36% by general surgeons, 39% by cardiothoracic surgeons, and 25% by noncardiac thoracic surgeons. Patient characteristics did not differ substantially by surgeon specialty. Adjusted operative mortality rates were lowest for cardiothoracic and noncardiac thoracic surgeons (7.6% general surgeons, 5.6% cardiothoracic surgeons, 5.8% noncardiac thoracic surgeons, P = 0.001). In analyses restricted to high-volume surgeons (>20 lung resections/y), mortality rates were lowest for noncardiac thoracic surgeons (5.1% noncardiac thoracic, 5.2% cardiothoracic, and 6.1% general surgeons) (P < 0.01 for difference between general surgeons and thoracic surgeons). In analyses restricted to high-volume hospitals (>45 lung resections/y), mortality rates were again lowest for noncardiac thoracic surgeons (5.0% noncardiac thoracic, 5.3% cardiothoracic, and 6.1% general surgeons) (P < 0.01 for differences between all 3 groups).
Conclusions: Operative mortality with lung resection varies by surgeon specialty. Some, but not all, of this variation in operative mortality is attributable to hospital and surgeon volume.
Figures
References
-
- Hannan EL, Popp AJ, Feustel P, et al. Association of surgical specialty and processes of care with patient outcomes for carotid endarterectomy. Stroke. 2001;32:2890–2897. - PubMed
-
- Reinbach DH, McGregor JR, Murray GD, et al. Effect of the surgeon's specialty interest on the type of resection performed for colorectal cancer. Dis Colon Rectum. 1994;37:1020–1023. - PubMed
-
- Read TE, Myerson RJ, Fleshman JW, et al. Surgeon specialty is associated with outcome in rectal cancer treatment. Dis Colon Rectum. 2002;45:904–914. - PubMed
-
- Dorrance HR, Docherty GM, O'Dwyer PJ. Effect of surgeon specialty interest on patient outcome after potentially curative colorectal cancer surgery. Dis Colon Rectum. 2000;43:492–498. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
