

Multiple, linked human immunodeficiency virus type 1 drug resistance mutations in treatment-experienced patients are missed by standard genotype analysis
- PMID: 15635002
- PMCID: PMC540111
- DOI: 10.1128/JCM.43.1.406-413.2005
Multiple, linked human immunodeficiency virus type 1 drug resistance mutations in treatment-experienced patients are missed by standard genotype analysis
Abstract
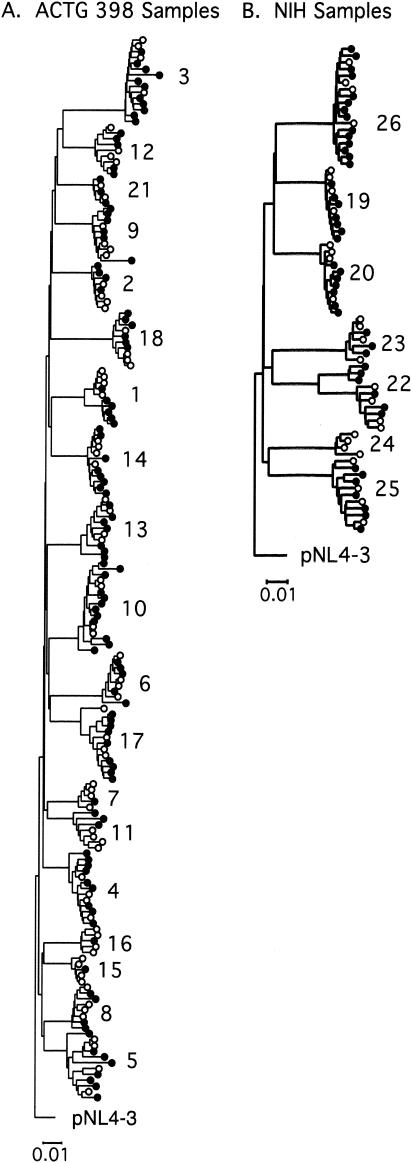
To investigate the extent to which drug resistance mutations are missed by standard genotyping methods, we analyzed the same plasma samples from 26 patients with suspected multidrug-resistant human immunodeficiency virus type 1 by using a newly developed single-genome sequencing technique and compared it to standard genotype analysis. Plasma samples were obtained from patients with prior exposure to at least two antiretroviral drug classes and who were on a failing antiretroviral regimen. Standard genotypes were obtained by reverse transcriptase (RT)-PCR and sequencing of the bulk PCR product. For single-genome sequencing, cDNA derived from plasma RNA was serially diluted to 1 copy per reaction, and a region encompassing p6, protease, and a portion of RT was amplified and sequenced. Sequences from 15 to 46 single viral genomes were obtained from each plasma sample. Drug resistance mutations identified by single-genome sequencing were not detected by standard genotype analysis in 24 of the 26 patients studied. Mutations present in less than 10% of single genomes were almost never detected in standard genotypes (1 of 86). Similarly, mutations present in 10 to 35% of single genomes were detected only 25% of the time in standard genotypes. For example, in one patient, 10 mutations identified by single-genome sequencing and conferring resistance to protease inhibitors (PIs), nucleoside analog reverse transcriptase inhibitors, and nonnucleoside reverse transcriptase inhibitors (NNRTIs) were not detected by standard genotyping methods. Each of these mutations was present in 5 to 20% of the 20 genomes analyzed; 15% of the genomes in this sample contained linked PI mutations, none of which were present in the standard genotype. In another patient sample, 33% of genomes contained five linked NNRTI resistance mutations, none of which were detected by standard genotype analysis. These findings illustrate the inadequacy of the standard genotype for detecting low-frequency drug resistance mutations. In addition to having greater sensitivity, single-genome sequencing identifies linked mutations that confer high-level drug resistance. Such linkage cannot be detected by standard genotype analysis.
Figures
References
-
- Albrecht, D., B. Zollner, H. H. Feucht, T. Lorenzen, R. Laufs, A. Stoehr, and A. Plettenberg. 2002. Reappearance of HIV multidrug-resistance in plasma and circulating lymphocytes after reintroduction of antiretroviral therapy. J. Clin. Virol. 24:93-98. - PubMed
-
- Bacheler, L. T., E. D. Anton, P. Kudish, D. Baker, J. Bunville, K. Krakowski, L. Bolling, M. Aujay, X. V. Wang, D. Ellis, M. F. Becker, A. L. Lasut, H. J. George, D. R. Spalding, G. Hollis, and K. Abremski. 2000. Human immunodeficiency virus type 1 mutations selected in patients failing efavirenz combination therapy. Antimicrob. Agents Chemother. 44:2475-2484. - PMC - PubMed
-
- Baxter, J. D., D. L. Mayers, D. N. Wentworth, J. D. Neaton, M. L. Hoover, M. A. Winters, S. B. Mannheimer, M. A. Thompson, D. I. Abrams, B. J. Brizz, J. P. Ioannidis, T. C. Merigan, et al. 2000. A randomized study of antiretroviral management based on plasma genotypic antiretroviral resistance testing in patients failing therapy. AIDS 14:F83-F93. - PubMed
-
- Brown, A. J., and A. Cleland. 1996. Independent evolution of the env and pol genes of HIV-1 during zidovudine therapy. AIDS 10:1067-1073. - PubMed
-
- Carpenter, C. C., M. A. Fischl, S. M. Hammer, M. S. Hirsch, D. M. Jacobsen, D. A. Katzenstein, J. S. Montaner, D. D. Richman, M. S. Saag, R. T. Schooley, M. A. Thompson, S. Vella, P. G. Yeni, and P. A. Volberding. 1997. Antiretroviral therapy for HIV infection in 1997. Updated recommendations of the International AIDS Society-USA panel. JAMA 277:1962-1969. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
