

Contrasting anesthetic sensitivities of T-type Ca2+ channels of reticular thalamic neurons and recombinant Ca(v)3.3 channels
- PMID: 15644869
- PMCID: PMC1575974
- DOI: 10.1038/sj.bjp.0706020
Contrasting anesthetic sensitivities of T-type Ca2+ channels of reticular thalamic neurons and recombinant Ca(v)3.3 channels
Abstract
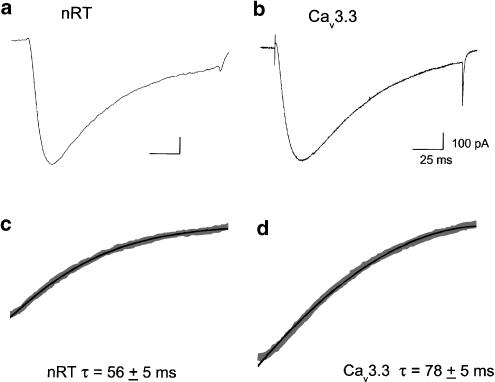
Reticular thalamocortical neurons express a slowly inactivating T-type Ca(2+) current that is quite similar to that recorded from recombinant Ca(v)3.3b (alpha1Ib) channels. These neurons also express abundant Ca(v)3.3 mRNA, suggesting that it underlies the native current. Here, we test this hypothesis by comparing the anesthetic sensitivities of recombinant Ca(v)3.3b channels stably expressed in HEK 293 cells to native T channels in reticular thalamic neurons (nRT) from brain slices of young rats. Barbiturates completely blocked both Ca(v)3.3 and nRT currents, with pentobarbital being about twice more potent in blocking Ca(v)3.3 currents. Isoflurane had about the same potency in blocking Ca(v)3.3 and nRT currents, but enflurane, etomidate, propofol, and ethanol exhibited 2-4 fold higher potency in blocking nRT vs Ca(v)3.3 currents. Nitrous oxide (N(2)O; laughing gas) blocked completely nRT currents with IC(50) of 20%, but did not significantly affect Ca(v)3.3 currents at four-fold higher concentrations. In addition, we observed that in lower concentration, N(2)O reversibly increased nRT but not Ca(v)3.3 currents. In conclusion, contrasting anesthetic sensitivities of Ca(v)3.3 and nRT T-type Ca(2+) channels strongly suggest that different molecular structures of Ca(2+) channels give rise to slowly inactivating T-type Ca(2+) currents. Furthermore, effects of volatile anesthetics and ethanol on slowly inactivating T-type Ca(2+) channel variants may contribute to the clinical effects of these agents.
Figures






References
-
- BARASH P.G., CULLEN B.F., STOELTING R.K.Neurophysiology and neuroanesthesia Clinical Anesthesia 1992Philadelphia: J.B. Lippincott; 871–918.2nd edn. ed. BENDO, A.A. pp
-
- BOSNJAK Z.J., SUPAN F.D., RUSCH N.J. The effects of halothane, enflurane, and isoflurane on calcium current in isolated canine ventricular cells. Anesthesiology. 1991;74:340–345. - PubMed
-
- CATLIN M.C., GUIZZETTI M., COSTA L.G. Effects of ethanol on calcium homeostasis in the nervous system: implications for astrocytes. Mol. Neurobiol. 1999;19:1–24. - PubMed
-
- CRIBBS L.L., LEE J.H., YANG J., SATIN J., ZHANG Y., DAUD A., BARCLAY J., WILLIAMSON M.P., FOX M., REES M., PEREZ-REYES E. Cloning and characterization of α1H from human heart, a member of the T-type Ca2+ channel gene family. Circ. Res. 1998;83:103–109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
