

Magnetic resonance colonography for the detection of inflammatory diseases of the large bowel: quantifying the inflammatory activity
- PMID: 15647191
- PMCID: PMC1774838
- DOI: 10.1136/gut.2003.037085
Magnetic resonance colonography for the detection of inflammatory diseases of the large bowel: quantifying the inflammatory activity
Abstract
Introduction: The purpose of this study was to assess the diagnostic accuracy of magnetic resonance colonography (MRC) for its ability to detect and quantify inflammatory bowel disease (IBD) affecting the colon. Endoscopically obtained histopathology specimens were used as the standard of reference.
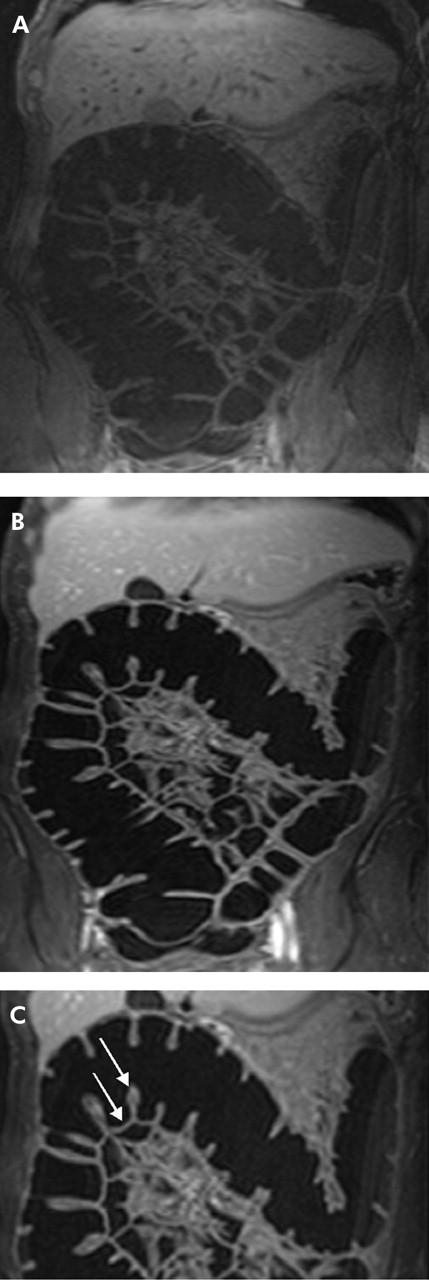
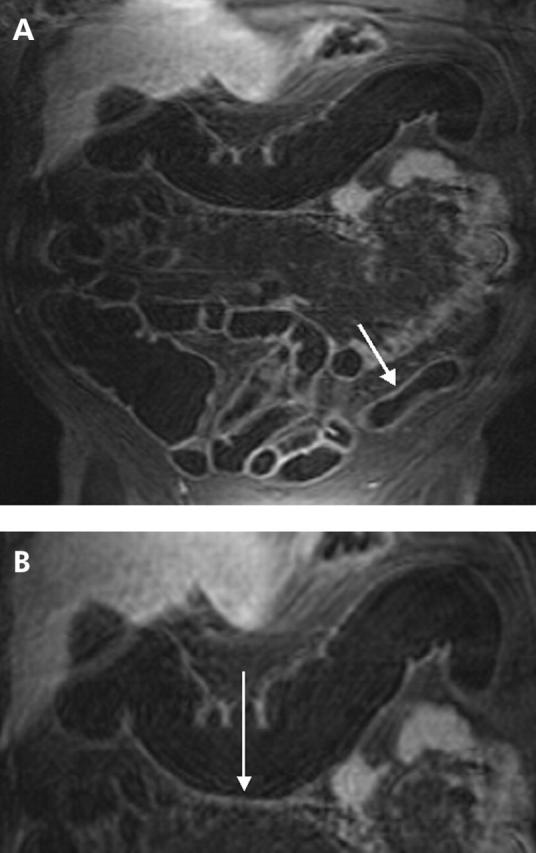
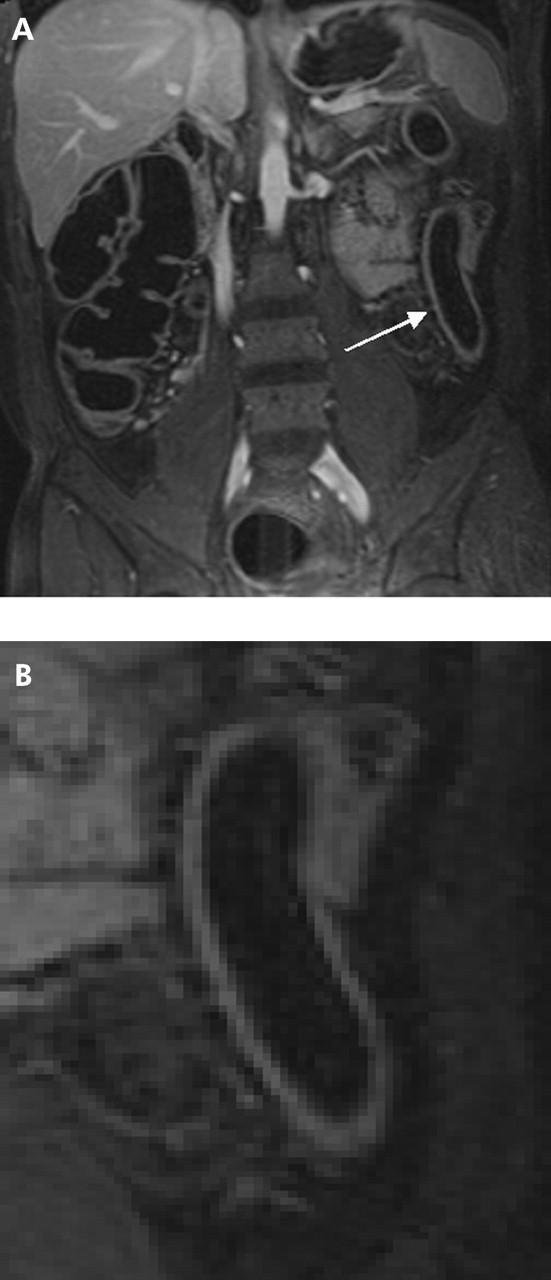
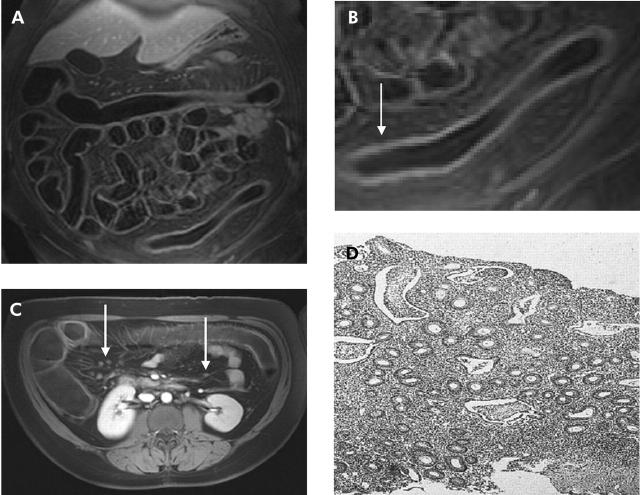
Materials and methods: Fifteen normal subjects and 23 patients with suspected IBD of the large bowel underwent MRC. Three dimensional T1 weighted data sets were collected following rectal administration of water prior to and 75 seconds after intravenous administration of paramagnetic contrast (gadolinium-BOPTA). The presence of inflammatory changes in patients was documented based on bowel wall contrast enhancement, bowel wall thickness, presence of perifocal lymph nodes, and loss of haustral folds. All four criteria were quantified relative to data obtained from normal subjects and summarised in a single score. This MRC based score was compared with histopathological data based on conventional endoscopic findings.
Results: MRC correctly identified 68 of 73 segments found to reveal IBD changes by histopathology. All severely inflamed segments were correctly identified as such and there were no false positive findings. Based on the proposed composite score, MRC detected and characterised clinically relevant IBD of the large bowel with sensitivity and specificity values of 87% and 100%, respectively, for all investigated colonic segments.
Conclusion: MRC may be considered a promising alternative to endoscopic biopsy in monitoring IBD activity or assessing therapeutic effectiveness.
Figures

Comment in
-
Value of MR colonography for assessment of inflammatory bowel disease? Believe what you see--see what you believe.Gut. 2005 Feb;54(2):181-2. doi: 10.1136/gut.2004.044982. Gut. 2005. PMID: 15647176 Free PMC article. No abstract available.
References
-
- Kiesslich R , Jung M, Galle PR, et al. Ulcerative colitis—how can endoscopic observation be improved? Dtsch Med Wochenschr 2003;128:139–41. - PubMed
-
- Nahon S , Bouhnik Y, Lavergne-Slove A, et al. Colonoscopy accurately predicts the anatomical severity of colonic Crohn’s disease attacks: correlation with findings from colectomy specimens. Am J Gastroenterol 2002;12:3102–7. - PubMed
-
- Eckardt VF, Gaedertz C, Eidner C. Colonic perforation with endoscopic biopsy. Gastrointest Endosc 1997;6:560–2. - PubMed
-
- Cappell MS, Friedel D. The role of sigmoidoscopy and colonoscopy in the diagnosis and management of lower gastrointestinal disorders: endoscopic findings, therapy, and complications. Med Clin North Am 2002;6:1253–88. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical