

Serum antibodies to carbonic anhydrase IV in patients with autoimmune pancreatitis
- PMID: 15647194
- PMCID: PMC1774835
- DOI: 10.1136/gut.2004.049064
Serum antibodies to carbonic anhydrase IV in patients with autoimmune pancreatitis
Abstract
Background and aims: Serum antibodies to carbonic anhydrase (CA) II have been reported in patients with autoimmune pancreatitis (AIP) and Sjogren's syndrome (SjS). However, their significance in the pathogenesis of these diseases is controversial. The aim of this study was to identify serum antibodies to CA isozymes, which are expressed in ductal cells of the pancreas.
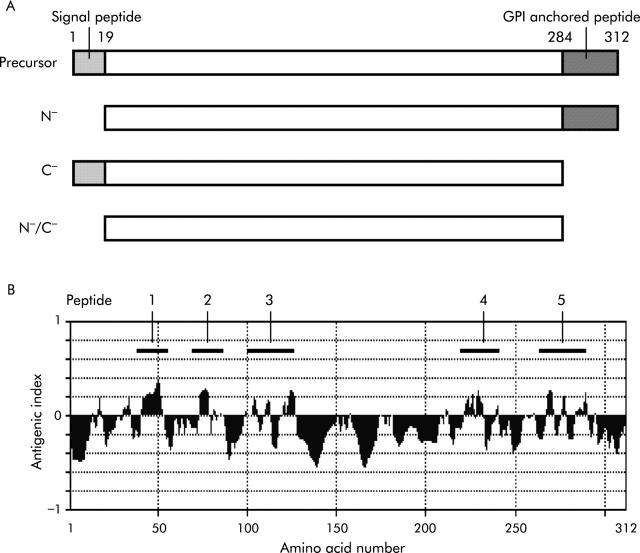
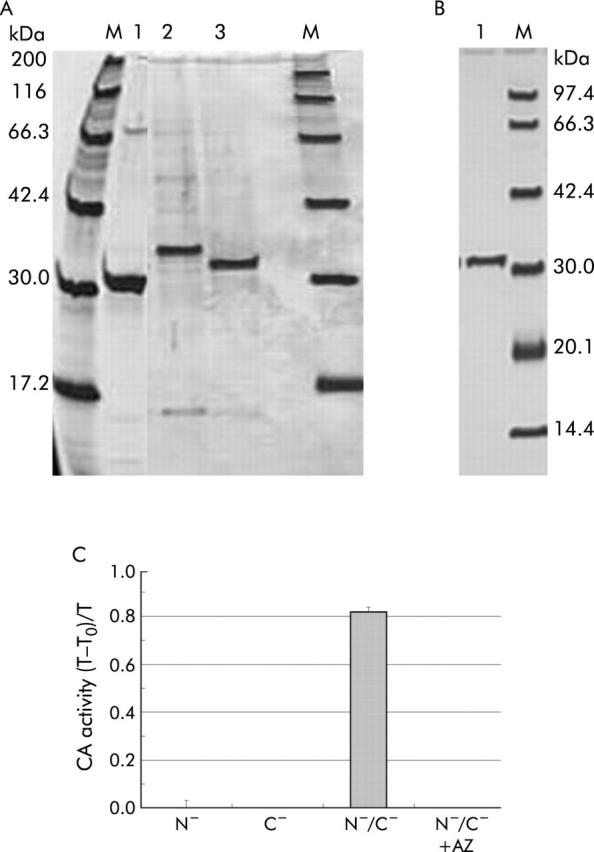
Methods: Recombinant proteins of human CAs IV, IX, and XII were obtained using a bacterial expression system, and five CA IV peptides with theoretically high antigenicity were synthesised. Western blotting and enzyme linked immunosorbent assay (ELISA) were used to detect serum antibodies to the CA isozymes.
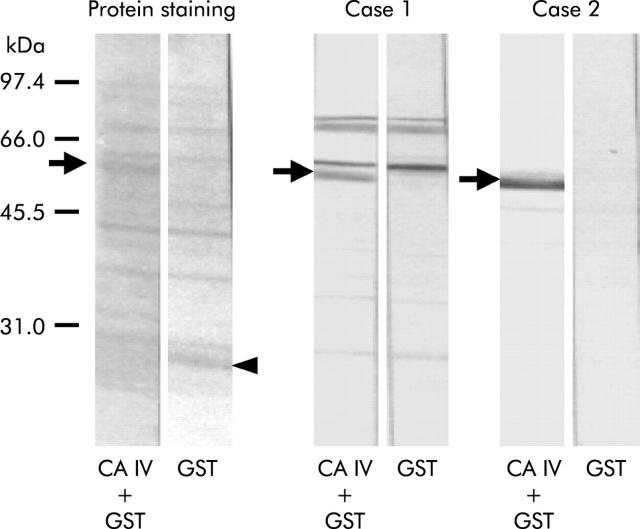
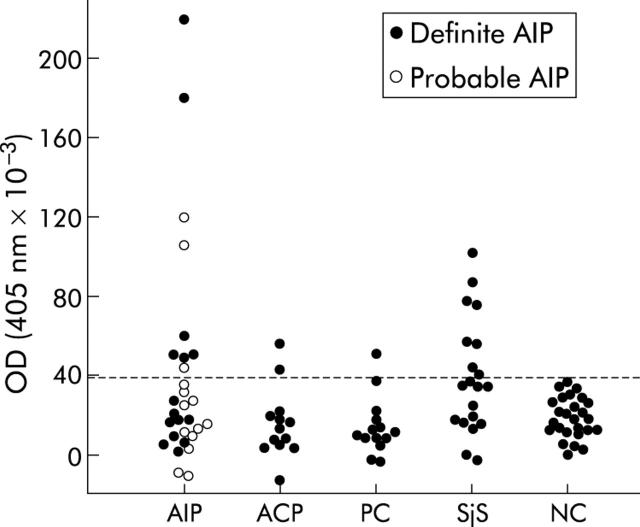
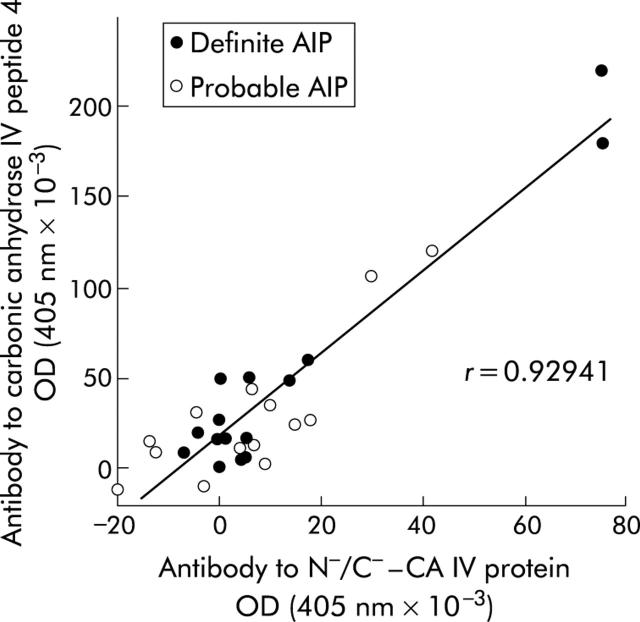
Results: The first screening analysis by western blot showed serum antibodies to CA IV among three CA isozymes in patients with idiopathic chronic pancreatitis, including AIP patients. Further analysis by ELISA showed a significantly increased prevalence of serum antibodies to the truncated CA IV protein and the CA IV synthetic peptide (LGS LTT PTC DEK VVW TVF REP I) in patients with definite AIP (4/15 and 6/20, respectively; p<0.01), probable AIP (6/14 and 3/14; p<0.02), and SjS (9/20 and 8/40; p<0.001) compared with normal controls (0/26). There was no significant difference in the antibody prevalence rates between normal controls and patients with alcoholic chronic pancreatitis (2/15 in each) or pancreatic cancer (2/14 and 1/14, respectively). The presence of serum antibodies to the CA IV peptide showed significant correlations with serum gamma-globulin and IgG levels in AIP patients.
Conclusions: These findings suggest that CA IV may be a target antigen that is commonly expressed in epithelial cells of specific tissues involved in AIP and its related diseases.
Figures
Comment in
-
Lack of serum antibodies to membrane bound carbonic anhydrase IV in patients with primary biliary cirrhosis.Gut. 2005 Nov;54(11):1665. doi: 10.1136/gut.2005.072389. Gut. 2005. PMID: 16227372 Free PMC article. No abstract available.
Similar articles
-
Serum antibodies to carbonic anhydrase I and II in patients with idiopathic chronic pancreatitis and Sjögren's syndrome.Gastroenterology. 1996 May;110(5):1579-86. doi: 10.1053/gast.1996.v110.pm8613065. Gastroenterology. 1996. PMID: 8613065
-
Potential for differential diagnosis of autoimmune pancreatitis and pancreatic cancer using carbonic anhydrase II antibody.Pancreas. 2008 Jul;37(1):e1-7. doi: 10.1097/MPA.0b013e318162cb3a. Pancreas. 2008. PMID: 18580434
-
Antibodies to carbonic anhydrase and IgG4 levels in idiopathic chronic pancreatitis: relevance for diagnosis of autoimmune pancreatitis.Gut. 2005 May;54(5):703-9. doi: 10.1136/gut.2004.047142. Gut. 2005. PMID: 15831920 Free PMC article.
-
The role of lymphotoxin signaling in the development of autoimmune pancreatitis and associated secondary extra-pancreatic pathologies.Cytokine Growth Factor Rev. 2014 Apr;25(2):125-37. doi: 10.1016/j.cytogfr.2014.01.003. Epub 2014 Jan 10. Cytokine Growth Factor Rev. 2014. PMID: 24508087 Review.
-
Carbonic anhydrase in human pancreas: hypotheses for the pathophysiological roles of CA isozymes.Ann N Y Acad Sci. 1999 Jun 30;880:5-16. doi: 10.1111/j.1749-6632.1999.tb09505.x. Ann N Y Acad Sci. 1999. PMID: 10415846 Review.
Cited by
-
Carbonic anhydrases as disease markers.Expert Opin Ther Pat. 2019 Jul;29(7):509-533. doi: 10.1080/13543776.2019.1629419. Epub 2019 Jun 17. Expert Opin Ther Pat. 2019. PMID: 31172829 Free PMC article. Review.
-
Autoimmune pancreatocholangitis, non-autoimmune pancreatitis and primary sclerosing cholangitis: a comparative morphological and immunological analysis.PLoS One. 2008 Jul 2;3(7):e2539. doi: 10.1371/journal.pone.0002539. PLoS One. 2008. PMID: 18596913 Free PMC article.
-
The Immunologic Paradoxes of IgG4-Related Disease.Clin Rev Allergy Immunol. 2018 Apr;54(2):344-351. doi: 10.1007/s12016-018-8679-y. Clin Rev Allergy Immunol. 2018. PMID: 29460058 Review.
-
IgG4- related disease: an orphan disease with many faces.Orphanet J Rare Dis. 2014 Jul 16;9:110. doi: 10.1186/s13023-014-0110-z. Orphanet J Rare Dis. 2014. PMID: 25026959 Free PMC article.
-
IgG4 Cholangiopathy.Int J Hepatol. 2012;2012:472376. doi: 10.1155/2012/472376. Epub 2011 Aug 4. Int J Hepatol. 2012. PMID: 21994885 Free PMC article.
References
-
- Ito T , Nakano I, Koyanagi S, et al. Autoimmune pancreatitis as a new clinical entity. Three cases of autoimmune pancreatitis with effective steroid therapy. Dig Dis Sci 1997;42:1458–68. - PubMed
-
- Yoshida K , Toki F, Takeuchi T, et al. Chronic pancreatitis caused by an autoimmune abnormality. Dig Dis Sci 1995;40:1561–8. - PubMed
-
- Cavallini G , Frulloni L. Autoimmunity and chronic pancreatitis: a concealed relationship. JOP 2001;2:61–8. - PubMed
-
- Kloppel G , Luttges J, Lohr M, et al. Autoimmune pancreatitis: pathological, clinical, and immunological features. Pancreas 2003;27:14–19. - PubMed
-
- Hayakawa T , Naruse S, Kitagawa M, et al. Clinical aspects of autoimmune pancreatitis in Sjogren’s syndrome. JOP 2001;2:88–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous