

The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection
- PMID: 15647196
- PMCID: PMC1774834
- DOI: 10.1136/gut.2004.046524
The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection
Abstract
Background and aims: Major liver resection incurs a risk of postoperative liver dysfunction and infection and there is a lack of objective evidence relating residual liver volume to these complications.
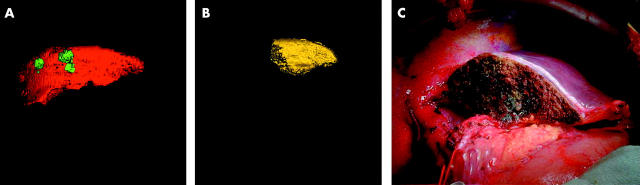
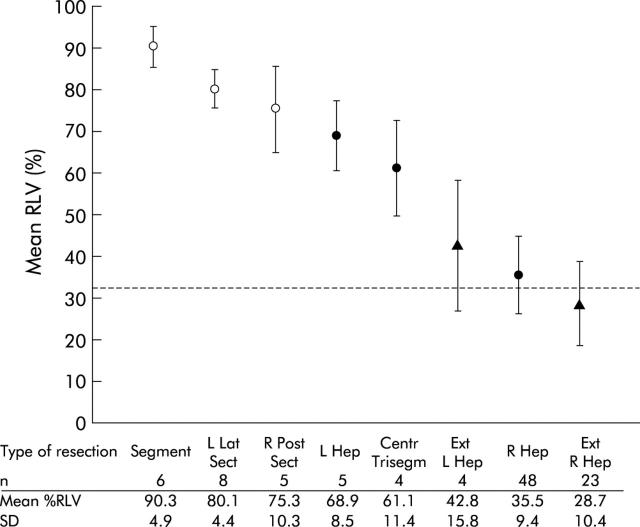
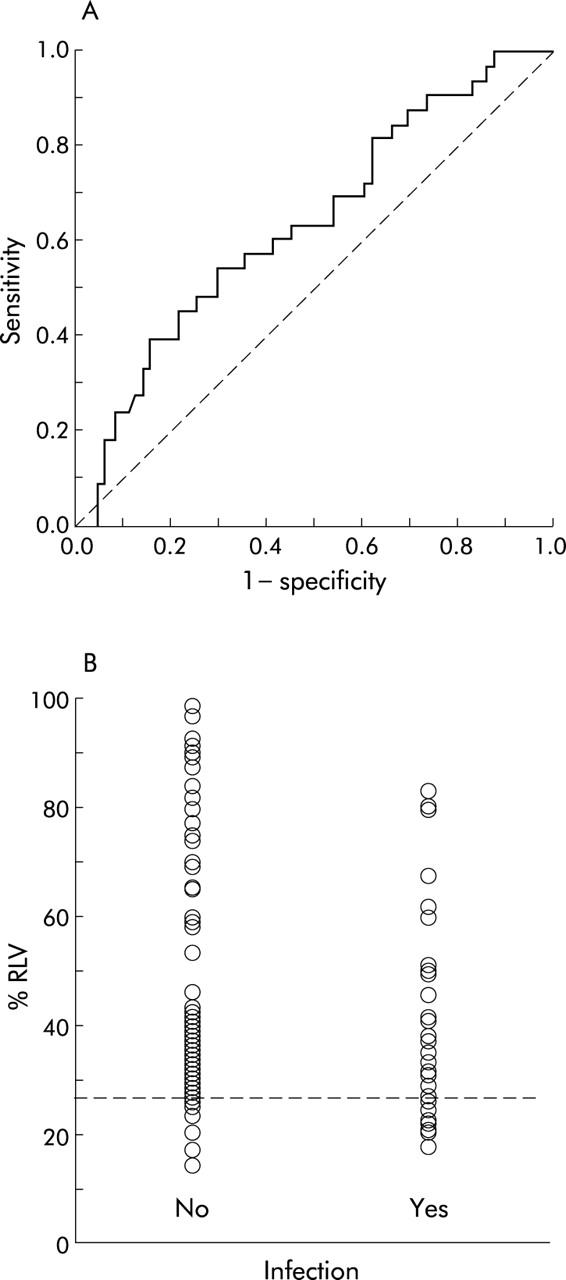
Patients and methods: Liver volumetry was performed on computer models derived from computed tomography (CT) angioportograms of 104 patients with normal synthetic liver function scheduled for liver resection. Relative residual liver volume (%RLV) was calculated as the relation of residual to total functional liver volume and related to postoperative hepatic dysfunction and infection. Receiver operator characteristic curve analysis was undertaken to determine the critical %RLV predicting severe hepatic dysfunction and infection. Univariate analysis and multivariate logistic regression analysis were performed to delineate perioperative predictors of severe hepatic dysfunction and infection.
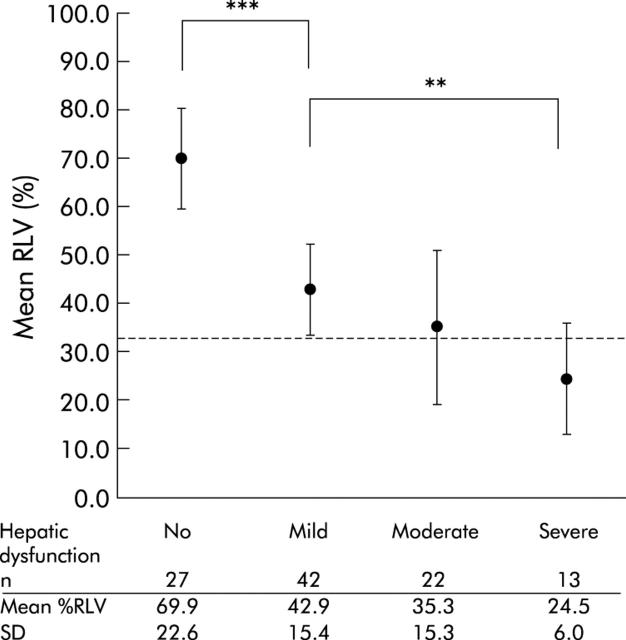
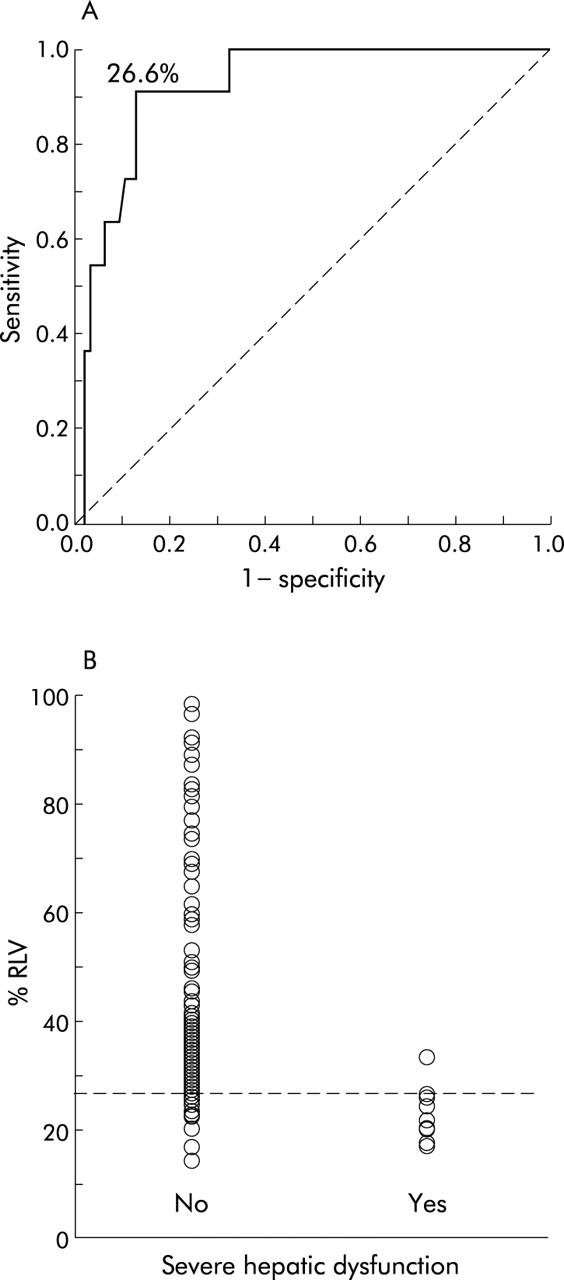
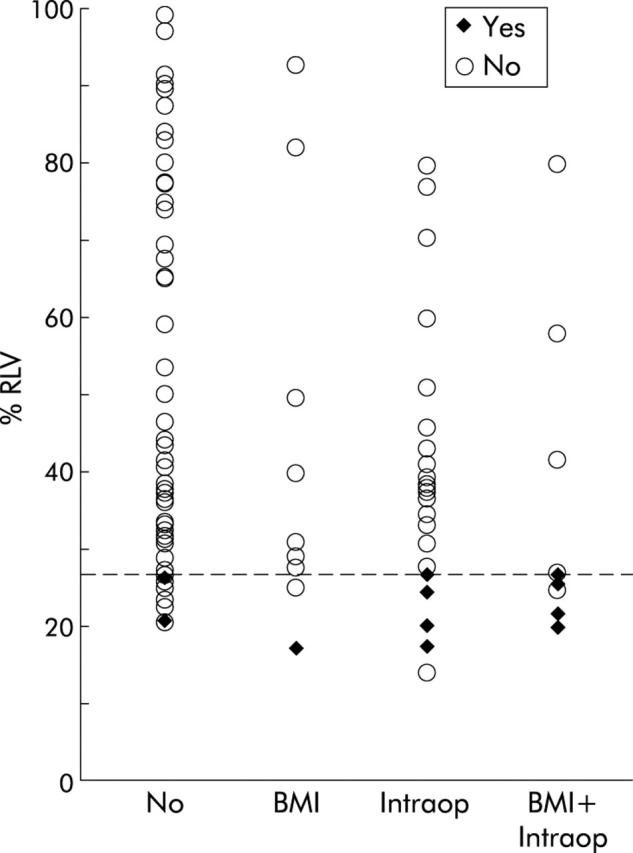
Results: The incidence of severe hepatic dysfunction and infection following liver resection increased significantly with smaller %RLV. A critical %RLV of 26.6% was identified as associated with severe hepatic dysfunction (p<0.0001). Additionally, body mass index (BMI), operating time, and intraoperative blood loss were significant prognostic indicators for severe hepatic dysfunction. It was not possible to predict the individual risk of postoperative infection precisely by %RLV. However, in patients undergoing major liver resection, infection was significantly more common in those who developed postoperative severe hepatic dysfunction compared with those who did not (p=0.030).
Conclusions: The likelihood of severe hepatic dysfunction following liver resection can be predicted by a small %RLV and a high BMI whereas postoperative infection is more related to liver dysfunction than precise residual liver volume. Understanding the relationship between liver volume and synthetic and immune function is the key to improving the safety of major liver resection.
Figures
References
-
- Jaeck D , Bachellier P, Guiguet M, et al. Long-term survival following resection of colorectal hepatic metastases. Association Francaise de Chirurgie. Br J Surg 1997;84:977–80. - PubMed
-
- Jamison RL, Donohue JH, Nagorney DM, et al. Hepatic resection for metastatic colorectal cancer results in cure for some patients. Arch Surg 1997;132:505–10. - PubMed
-
- Rees M , Plant G, Bygrave S. Late results justify resection for multiple hepatic metastases from colorectal cancer. Br J Surg 1997;84:1136–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical