

ATP flux through creatine kinase in the normal, stressed, and failing human heart
- PMID: 15647364
- PMCID: PMC545546
- DOI: 10.1073/pnas.0408962102
ATP flux through creatine kinase in the normal, stressed, and failing human heart
Abstract
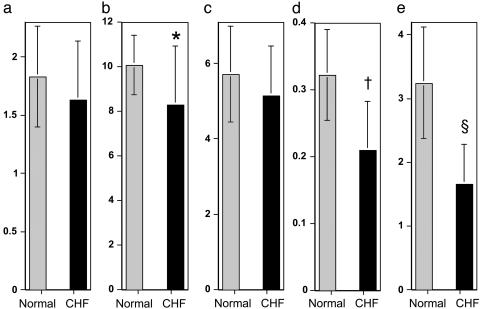
The heart consumes more energy per gram than any other organ, and the creatine kinase (CK) reaction serves as its prime energy reserve. Because chemical energy is required to fuel systolic and diastolic function, the question of whether the failing heart is "energy starved" has been debated for decades. Despite the central role of the CK reaction in cardiac energy metabolism, direct measures of CK flux in the beating human heart were not previously possible. Using an image-guided molecular assessment of endogenous ATP turnover, we directly measured ATP flux through CK in normal, stressed, and failing human hearts. We show that cardiac CK flux in healthy humans is faster than that estimated through oxidative phosphorylation and that CK flux does not increase during a doubling of the heart rate-blood pressure product by dobutamine. Furthermore, cardiac ATP flux through CK is reduced by 50% in mild-to-moderate human heart failure (1.6 +/- 0.6 vs. 3.2 +/- 0.9 micromol/g of wet weight per sec, P <0.0005). We conclude that magnetic resonance strategies can now directly assess human myocardial CK energy flux. The deficit in ATP supplied by CK in the failing heart is cardiac-specific and potentially of sufficient magnitude, even in the absence of a significant reduction in ATP stores, to contribute to the pathophysiology of human heart failure. These findings support the pursuit of new therapies that reduce energy demand and/or augment energy transfer in heart failure and indicate that cardiac magnetic resonance can be used to assess their effectiveness.
Figures


References
-
- Ingwall, J. S. (1993) Circulation 87, VII58-VII62.
-
- Katz, A. M. (1998) Cardiol. Clin. 16, 633-644. - PubMed
-
- Poole-Wilson, P. A. (2002) J. Am. Med. Assoc. 287, 1578-1580. - PubMed
-
- Ingwall, J. S., Kramer, M. F., Fifer, M. A., Lorell, B. H., Shemin, R., Grossman, W. & Allen, P. D. (1985) N. Engl. J. Med. 313, 1050-1054. - PubMed
-
- Wallimann, T. (1994) Curr. Biol. 4, 42-46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
