

Noninvasive sudden death risk stratification by ambulatory ECG-based T-wave alternans analysis: evidence and methodological guidelines
- PMID: 15649246
- PMCID: PMC6931922
- DOI: 10.1111/j.1542-474X.2005.10103.x
Noninvasive sudden death risk stratification by ambulatory ECG-based T-wave alternans analysis: evidence and methodological guidelines
Abstract
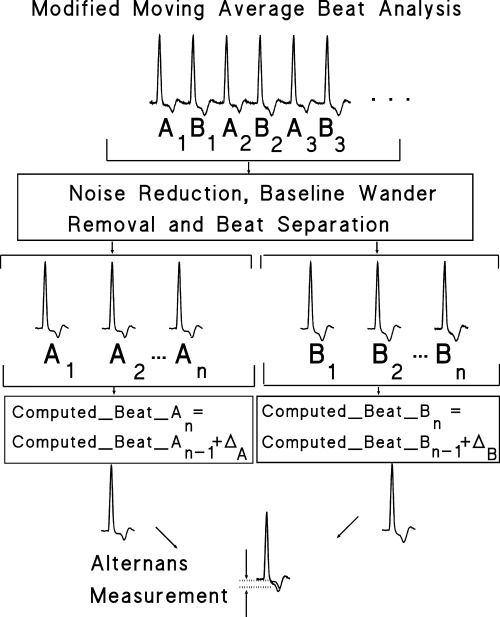
Extensive experimental and clinical evidence supports the utility of T-wave alternans (TWA) as a marker of risk for ventricular fibrillation. This entity appears to reflect the fundamental arrhythmogenic property of enhanced dispersion of repolarization. This relationship probably accounts for its relative ubiquity in patients with diverse types of cardiac disease, as has been recognized with the development of analytical tools. A basic premise of this review is that ambulatory ECG monitoring of TWA as patients experience the provocative stimuli of daily activities can expose latent electrical instability in individuals at heightened risk for arrhythmias. We will discuss the literature that supports this concept and summarize the current state of knowledge regarding the use of routine ambulatory ECGs to evaluate TWA for arrhythmia risk stratification. The dynamic, nonspectral modified moving average analysis method for assessing TWA, which is compatible with ambulatory ECG monitoring, is described along with methodological guidelines for its implementation. Finally, the rationale for combined monitoring of autonomic markers along with TWA will be presented.
Figures
References
-
- Konta T, Ikeda K, Yamaki M, et al Significance of discordant ST alternans in ventricular fibrillation. Circulation 1990;82: 2185–2189. - PubMed
-
- Surawicz B, Fisch C. Cardiac alternans: Diverse mechanisms and clinical manifestations. J Am Coll Cardiol 1992;20: 483–499. - PubMed
-
- Nearing BD, Verrier RL. Tracking heightened cardiac electrical instability by computing interlead heterogeneity of T‐wave morphology. J Appl Physiol 2003;95: 2265–2272. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
