

Assessment of acute spinal inflammation in patients with ankylosing spondylitis by magnetic resonance imaging: a comparison between contrast enhanced T1 and short tau inversion recovery (STIR) sequences
- PMID: 15650011
- PMCID: PMC1755589
- DOI: 10.1136/ard.2004.031609
Assessment of acute spinal inflammation in patients with ankylosing spondylitis by magnetic resonance imaging: a comparison between contrast enhanced T1 and short tau inversion recovery (STIR) sequences
Abstract
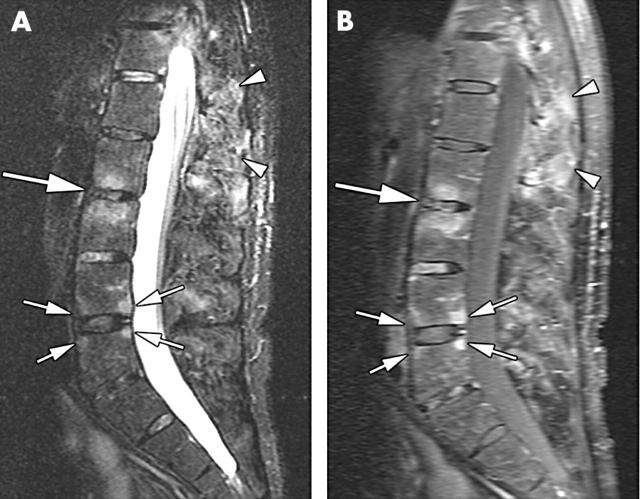
Objectives: To compare the performance of two different MRI sequences-T(1) weighted, fat saturated, spin echo after application of contrast medium, and short tau inversion recovery (STIR) sequences-to detect spinal inflammation in patients with ankylosing spondylitis (AS).
Methods: Both MRI sequences were performed in 38 patients with active AS and compared using the MRI activity scoring system, ASspiMRI-a. One vertebral unit (VU) was defined as the region between two virtual lines drawn through the middle of each vertebral body.
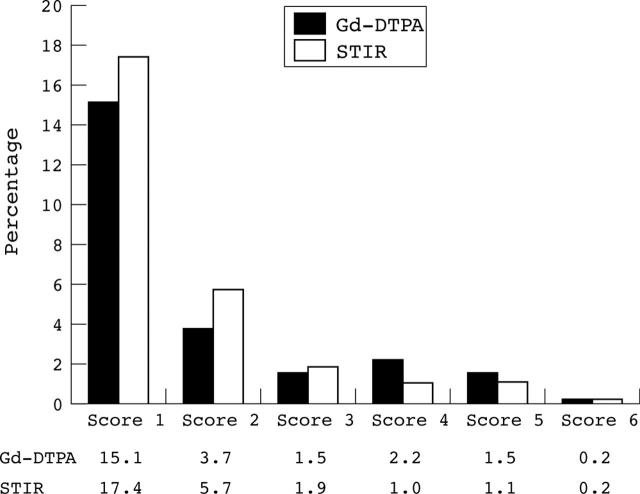
Results: Intraclass correlation coefficients were excellent-0.91 and 0.86 for the Gd-DTPA and STIR sequences, respectively. The overall correlation of the single MRI scores for both sequences was also good (r = 0.84, p = 0.01). The intrarater variance was 6.71 and 9.41 and the interrater variance was 13.16 and 19.04 for the Gd-DTPA and STIR sequences, respectively. The smallest detectable distance was 4.7 and 5.6 for the Gd-DTPA and STIR sequences, respectively. The concordance rate for both sequences was 83.5% (range 80.5-87.7% in the three spinal segments). Inflammatory spinal lesions were found in 10.1% of the VUs in the STIR sequence but not in the T(1)/Gd-DTPA sequence, while the T(1)/Gd-DTPA sequence showed inflammatory lesions in 6.4% of the VUs that were found normal by STIR.
Conclusions: Both MRI techniques can evaluate active spinal lesions in patients with AS. More spinal lesions are detected by the STIR sequence, but the reliability between readings and readers is better for the Gd-DTPA sequence. The ASspiMRI-a is a reliable instrument for evaluating acute spinal changes in AS.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
