

H-graft portacaval shunts versus TIPS: ten-year follow-up of a randomized trial with comparison to predicted survivals
- PMID: 15650633
- PMCID: PMC1356908
- DOI: 10.1097/01.sla.0000151884.67600.b6
H-graft portacaval shunts versus TIPS: ten-year follow-up of a randomized trial with comparison to predicted survivals
Abstract
Objective: To report long-term outcome of patients undergoing prosthetic 8-mm H-graft portacaval shunts (HGPCS) or TIPS and to compare actual with predicted survival data.
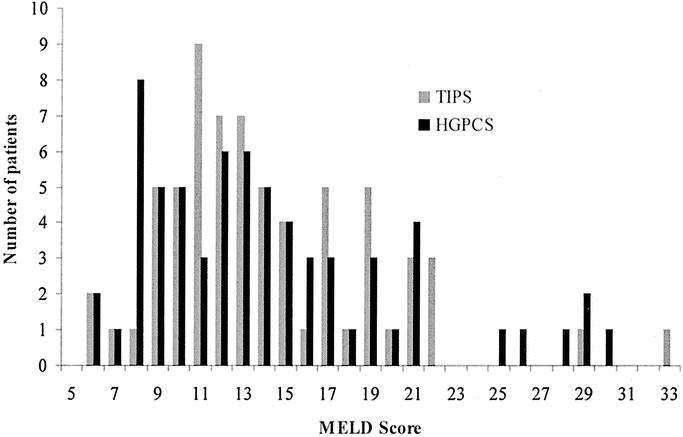
Methods: A randomized trial comparing TIPS to HGPCS for bleeding varices began in 1993. Predicted survival was determined using MELD (Model for End-stage Liver Disease).
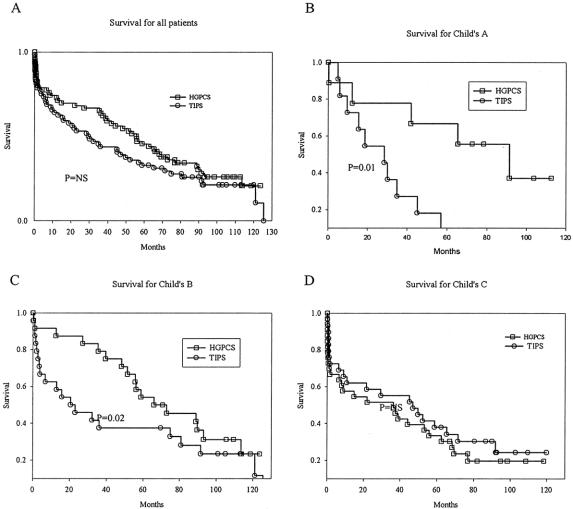
Results: Patients undergoing TIPS (N = 66) or HGPCS (N = 66) were very similar by Child's class and MELD scores and predicted survival. After TIPS (P = 0.01) and HGPCS (P = 0.001), actual survival was superior to predicted survival. Through 24 months, actual survival after HGPCS was superior to actual survival after TIPS (P = 0.04). Compared with TIPS, survival was superior after HGPCS for patients of Child's class A and B (P = 0.07) and with MELD scores less than 13 (P = 0.04) with follow-up at 5 to 10 years. Shunt failure was less following HGPCS (P < 0.01).
Conclusions: Predicted survival data for patients undergoing TIPS or HGPCS confirms an unbiased randomization. Actual survival following TIPS or HGPCS was superior to predicted survival. Shunt failure favored HGPCS, as did survival after shunting, particularly for the first few years after shunting and for patients of Child's class A or B or with MELD scores less than 13. This trial irrefutably establishes a role for surgical shunting, particularly HGPCS.
Figures
References
-
- Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
-
- Malinchoc M, Kamath PS, Gordon FD, et al. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000;31:864–871. - PubMed
-
- Ferral H, Gamboa P, Postoak DW, et al. Survival after elective transjugular intrahepatic portosystemic shunt creation: prediction with model for end-stage liver disease score. Radiology. 2004;231:231–236. - PubMed
-
- Rosemurgy AS, Serafini FM, Zweibel BR, et al. Transjugular intrahepatic portosystemic shunt vs. small-diameter prosthetic H-graft portacaval shunt: extended follow-up of an expanded randomized prospective trial. J Gastrointest Surg. 2000;4:589–597. - PubMed
-
- Rosemurgy AS. Small diameter interposition shunt. In: Nyhus L, Baker R, Fischer J, eds. Mastery of Surgery. Boston: Little, Brown, 1997:1301–1307.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
