

Evaluation of the learning curve in ileal pouch-anal anastomosis surgery
- PMID: 15650636
- PMCID: PMC1356911
- DOI: 10.1097/01.sla.0000152018.99541.f1
Evaluation of the learning curve in ileal pouch-anal anastomosis surgery
Abstract
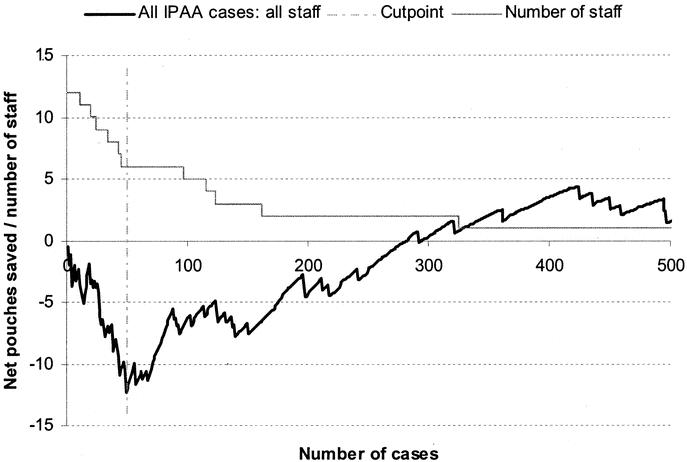
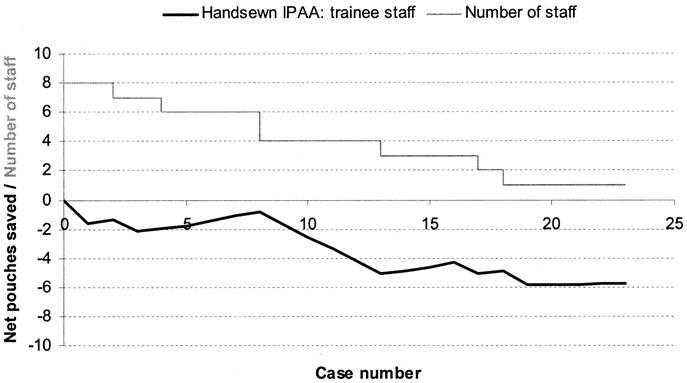
Summary background data: We define the learning curve required to attain satisfactory training in ileal pouch-anal anastomosis (IPAA) and identify possible differences in the learning curve for stapled and hand-sewn IPAA surgery. Various studies have addressed the differences in failure rate between stapled and hand-sewn IPAA, but there is no literature that evaluates the differences in attaining satisfactory training in each of these techniques.
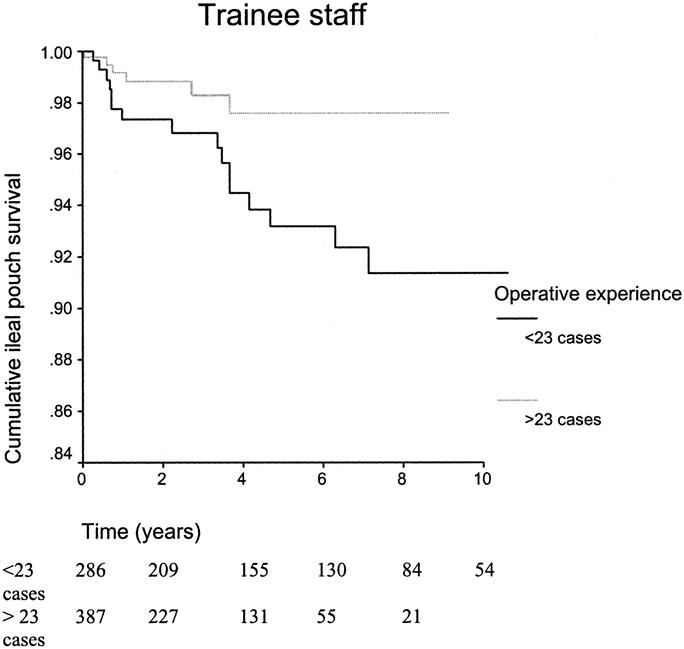
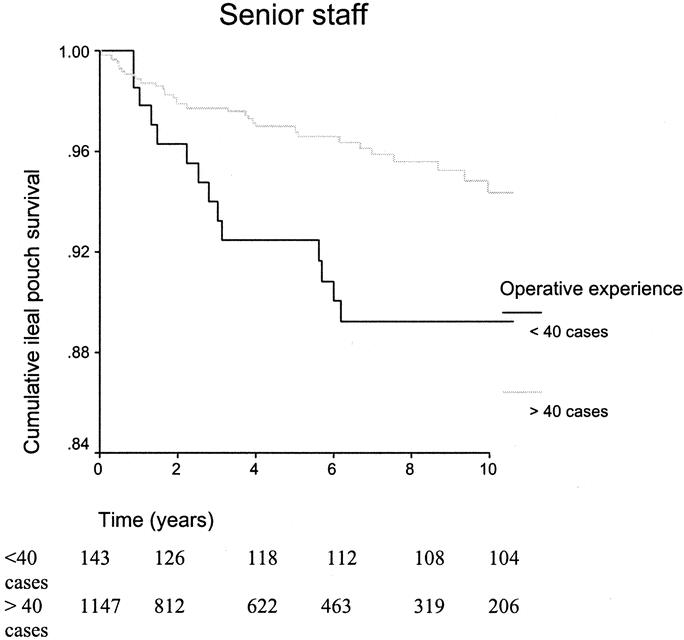
Methods: Data were collected from 1965 patients undergoing IPAA surgery by 12 surgeons in a single center between 1983 and 2001. Using ileoanal pouch failure as the primary end point, a parametric survival model was used to adjust for case mix (patient comorbidity, preoperative diagnosis, manometric findings, and prior anal pathology). A risk-adjusted cumulative sum (CUSUM) model was used for monitoring outcomes in IPAA surgery.
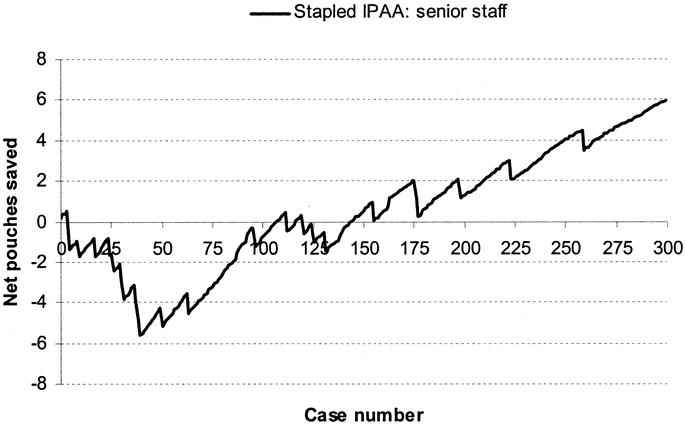
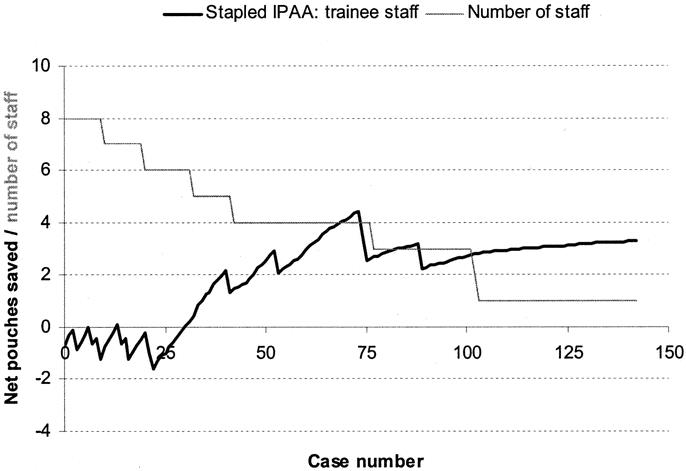
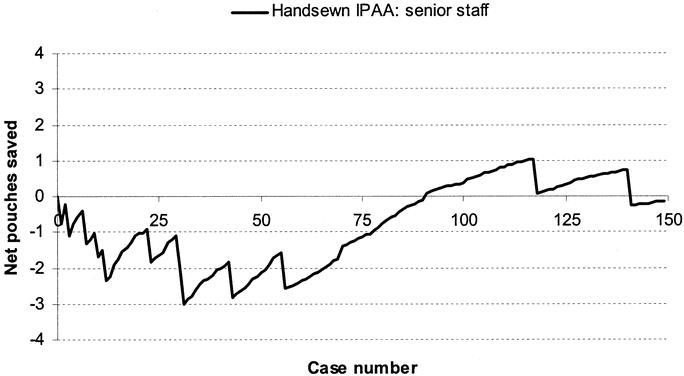
Results: The 5-year ileal pouch survival was 95.6% (median patient follow-up of 4.2 years; range 0-19 years). Fifty percent of trainee staff demonstrated a learning curve in IPAA surgery. Having adjusted for case mix, trainee staff undertaking stapled IPAA surgery showed an improvement in the pouch failure rate following an initial training period of 23 cases versus 40 cases for senior staff. The learning curve for hand-sewn IPAA surgery was quantified only for senior staff who attained adequate results following an initial period of 31 procedures.
Conclusions: The CUSUM method was a useful tool for objectively measuring performance during the learning phase of IPAA surgery. With adequate training, supervision, and monitoring, the learning curve in IPAA surgery may be reduced even further.
Figures
References
-
- Ramsay CR, Wallace SA, Garthwaite PH, et al. Assessing the learning curve effect in health technologies: lessons from the nonclinical literature. Int J Technol Assess Health Care. 2002;18:1–10. - PubMed
-
- Ramsay CR, Grant AM, Wallace SA, et al. Assessment of the learning curve in health technologies: a systematic review. Int J Technol Assess Health Care. 2000;16:1095–108. - PubMed
-
- Novick RJ, Stitt LW. The learning curve of an academic cardiac surgeon: use of the CUSUM method. J Card Surg. 1999;14:312–320. - PubMed
-
- Van Rij AM, McDonald JR, Pettigrew RA, et al. CUSUM as an aid to early assessment of the surgical trainee. Br J Surg. 1995;82:1500–1503. - PubMed
-
- Wohl H. The cusum plot: its utility in the analysis of clinical data. N Engl J Med. 1977;296:1044–1045. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
