

Prognostic significance of preoperative [18-F] fluorodeoxyglucose (FDG) positron emission tomography (PET) imaging in patients with resectable soft tissue sarcomas
- PMID: 15650639
- PMCID: PMC1356914
- DOI: 10.1097/01.sla.0000152663.61348.6f
Prognostic significance of preoperative [18-F] fluorodeoxyglucose (FDG) positron emission tomography (PET) imaging in patients with resectable soft tissue sarcomas
Abstract
Objective: The objective of this study was to evaluate the prognostic significance of preoperative positron emission tomography (PET) using 2-fluoro-2-deoxy-D-glucose (FDG) by calculating the mean standardized uptake values (SUV) in patients with resectable soft tissue sarcomas (STS).
Summary and background data: FDG-PET might be used as an adjunctive tool (in addition to biopsy and radiologic tomography) in the preoperative prognostic assessment of resectable STS.
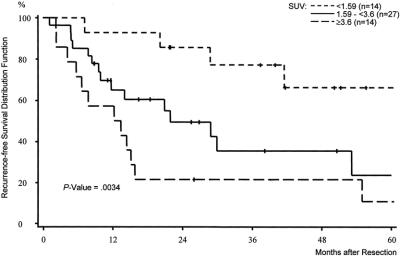
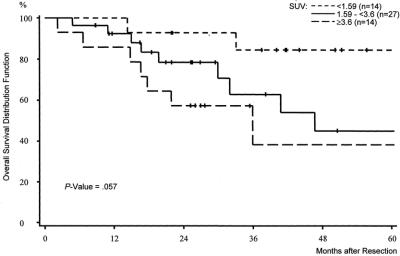
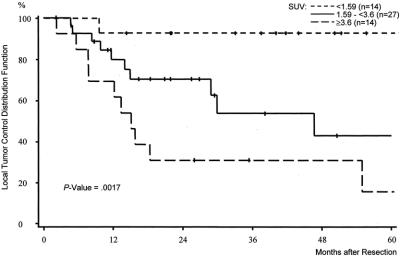
Methods: A total of 74 adult patients with STS underwent preoperative FDG-PET imaging with calculation of the SUV. Clinicopathologic data and the SUV were analyzed for an association with the clinical outcome. The first and the third quartiles of the SUV distribution function were used as cutoff values (1.59 and 3.6). Survival was estimated by the Kaplan-Meier method. Univariate and multivariate analyses were performed using log-rank test and the Cox proportional hazards regression model.
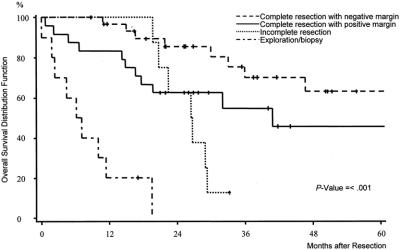
Results: In 55 cases, STS were completely resected (follow up 40 months): 5-year recurrence-free survival rates in patients with SUV <1.59, 1.59 to <3.6, and > or =3.6 were 66%, 24%, and 11%, respectively (P = 0.0034). SUV was a predictor for overall survival (5-year rates: 84% [SUV <1.59], 45% [SUV 1.59 to <3.6], and 38% [SUV > or =3.6]; P = 0.057) and local tumor control (5-year rates: 93% [SUV <1.59], 43% [SUV 1.59 to <3.6], and 15% [SUV > or =3.6]; P = 0.0017). By multivariate analysis, SUV was found to be predictive for recurrence-free survival. The prognostic differences with respect to the SUV were associated with tumor grade (P = 0.002).
Conclusion: The semiquantitative FDG uptake, as measured by the mean SUV on preoperative PET images in patients with resectable STS, is a useful prognostic parameter. SUV with cutoff values at the first and the third quartiles of the SUV distribution predicted overall survival, recurrence-free survival, and local tumor control. Therefore, FDG-PET can be used to improve the preoperative prognostic assessment in patients with resectable STS.
Figures
References
-
- Frassica FJ, Khanna JA, McCarthy EF. The role of MR imaging in soft tissue tumor evaluation: perspective of the orthopedic oncologist and musculoskeletal pathologist. Magn Reson Imaging Clin North Am. 2000;8:915–927. - PubMed
-
- De Schepper AM, De Beuckeleer L, Vandevenne J, et al. Magnetic resonance imaging of soft tissue tumors. Eur Radiol. 2000;10:213–223. - PubMed
-
- Imaizumi S, Morita T, Ogose A, et al. Soft tissue sarcoma mimicking chronic hematoma: value of magnetic resonance imaging in differential diagnosis. J Orthop Sci. 2002;7:33–37. - PubMed
-
- Jones C, Liu K, Hirschowitz S, et al. Concordance of histopathologic and cytologic grading in musculoskeletal sarcomas: can grades obtained from analysis of the fine-needle aspirates serve as the basis for therapeutic decisions? Cancer. 2002;96:83–91. - PubMed
-
- Hoeber I, Spillane AJ, Fisher C, et al. Accuracy of biopsy techniques for limb and limb girdle soft tissue tumors. Ann Surg Oncol. 2001;8:80–87. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
