

Histopathologic excision margin affects local recurrence rate: analysis of 2681 patients with melanomas < or =2 mm thick
- PMID: 15650644
- PMCID: PMC1356919
- DOI: 10.1097/01.sla.0000152014.89434.96
Histopathologic excision margin affects local recurrence rate: analysis of 2681 patients with melanomas < or =2 mm thick
Abstract
Objective: Prospective trials have shown that 1-cm and 2-cm margins are safe for melanomas <1 mm thick and > or =1 mm thick, respectively. It is unknown whether narrower margins increase the risk of LR or mortality.
Summary background data: To determine the relationship between histopathologic excision margin, local recurrence (LR) and survival for patients with melanomas < or =2 mm thick.
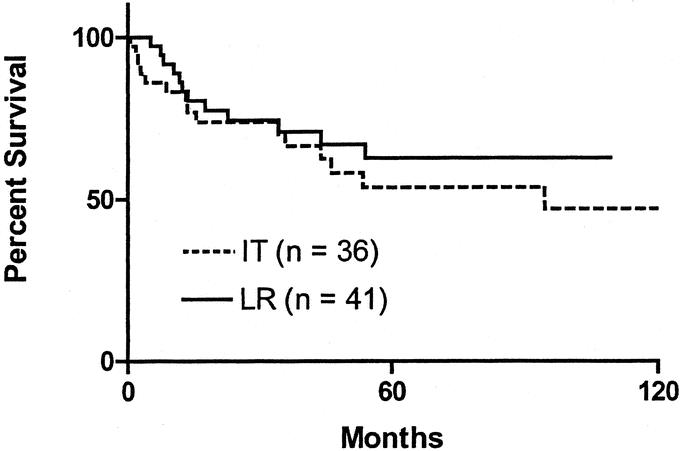
Methods: Data were extracted from the Sydney Melanoma Unit database for all patients with cutaneous melanoma < or =2 mm thick, diagnosed up to 1996. Patients with positive excision margins or follow-up <12 months were excluded, leaving 2681 for analysis. Outcome measures were LR (recurrence <5 cm from the excision scar), in-transit recurrence, and disease-specific survival. Factors predicting LR and overall survival were tested with Cox proportional hazards analysis.
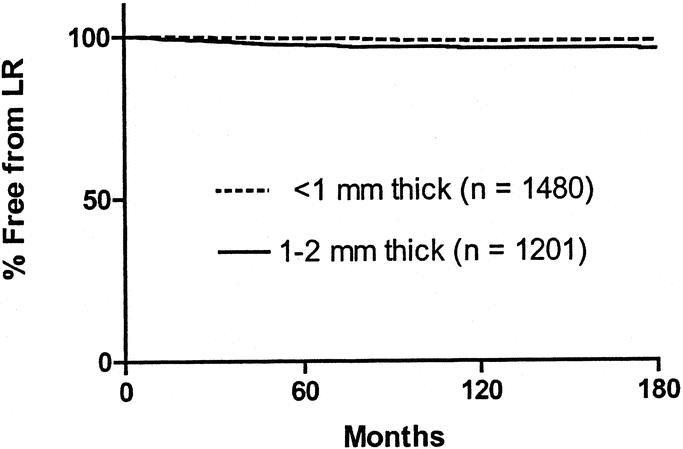
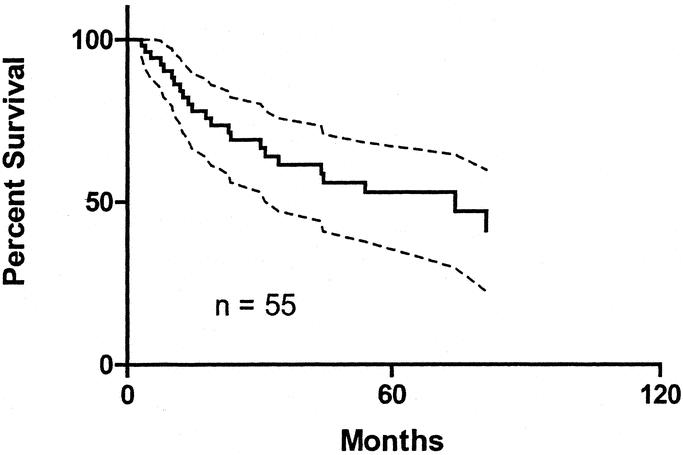
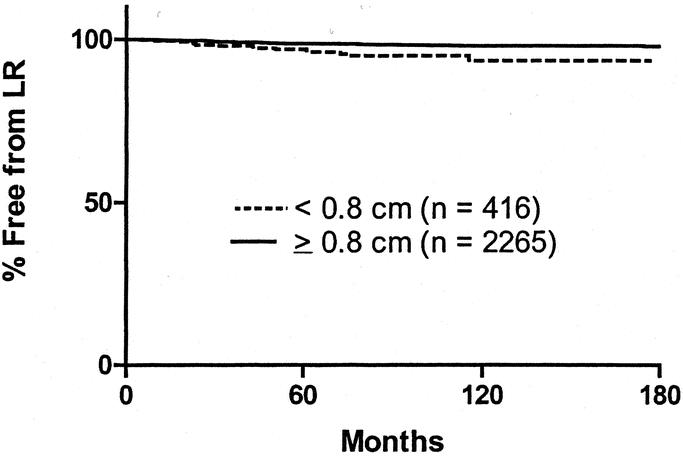
Results: Median follow-up was 83.8 months. LR was identified in 55 patients (median time to recurrence, 37 months). At 120 months, the actuarial LR rate was 2.9%. Five-year survival after LR was 52.8%. In multivariate analysis, only margin of excision and tumor thickness were predictive of LR (both P = 0.003). When all patients with a margin <0.8 cm in fixed tissue (corresponding to a margin of <1 cm in vivo) were excluded from analysis, margin was no longer significant in predicting LR. Thickness, ulceration, and site were predictive of survival, but margin was not (P = 0.49).
Conclusions: Histopathologic margin affects the risk of LR. However, if the in vivo margin is > or =1 cm, it no longer predicts risk of LR. Patient survival is not affected by margin.
Figures
Comment in
-
Histopathologic excision margin affects local recurrence rate: Analysis of 2681 patients with melanoma < or = 2 mm thick.Ann Surg. 2006 Apr;243(4):569; author reply 569-570. doi: 10.1097/01.sla.0000209150.32978.30. Ann Surg. 2006. PMID: 16552212 Free PMC article. No abstract available.
References
-
- Veronesi U, Cascinelli N. Narrow excision (1-cm margin): a safe procedure for thin cutaneous melanoma. Arch Surg. 1991;126:438–441. - PubMed
-
- Balch CM, Soong SJ, Smith T, et al. Long-term results of a prospective surgical trial comparing 2 cm vs. 4 cm excision margins for 740 patients with 1–4 mm melanomas. Ann Surg Oncol. 2001;8:101–108. - PubMed
-
- Ringborg U, Andersson R, Eldh J, et al. Resection margins of 2 versus 5 cm for cutaneous malignant melanoma with a tumor thickness of 0.8 to 2.0 mm: randomized study by the Swedish Melanoma Study Group. Cancer. 1996;77:1809–1814. - PubMed
-
- Khayat D, Rixe O, Martin G, et al. Surgical margins in cutaneous melanoma (2 cm versus 5 cm for lesions measuring less than 2.1-mm thick). Cancer. 2003;97:1941–1946. - PubMed
-
- Thomas JM, Newton-Bishop J, A'Hern R, et al. Excision margins in high-risk malignant melanoma. N Engl J Med. 2004;350:757–766. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
