

Report on financing the new model of family medicine
- PMID: 15654084
- PMCID: PMC1466777
- DOI: 10.1370/afm.237
Report on financing the new model of family medicine
Abstract
Purpose: To foster redesigning the work and workplaces of family physicians, this Future of Family Medicine task force was created to formulate and recommend a financial model that sustains and promotes a thriving New Model of care by focusing on practice reimbursement and health care finances. The goals of the task force were to develop a financial model that assesses the impact of the New Model on practice finances, and to recommend health care financial policies that, if implemented, would be expected to promote the New Model and the primary medical care function in the United States for the next few decades.
Methods: The members of the task force reflected a wide range of professional backgrounds and expertise. The group met in person on 2 occasions and communicated by e-mail and conference calls to achieve consensus. A marketing study was carried out using focus groups to test the concept of the New Model with consumers. External consultants with expertise in health economics, health care finance, health policy, and practice management were engaged to assist the task force with developing the microeconomic (practice level) and macroeconomic (societal level) financial models necessary to achieve its goals. Model assumptions were derived from the published medical literature, existing practice management databases, and discussions with experienced physicians and other content experts. The results of the financial modeling exercise are included in this report. The initial draft report of the findings and recommendations was shared with a reactor panel representing a broad spectrum of constituencies. Feedback from these individuals was reviewed and incorporated, as appropriate, into the final report.
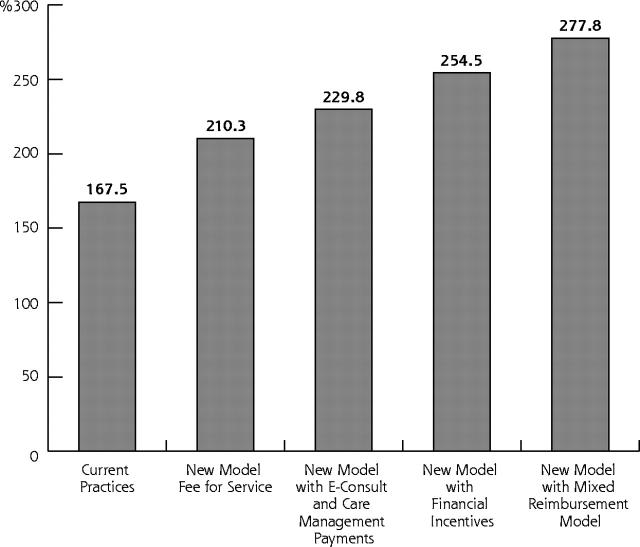
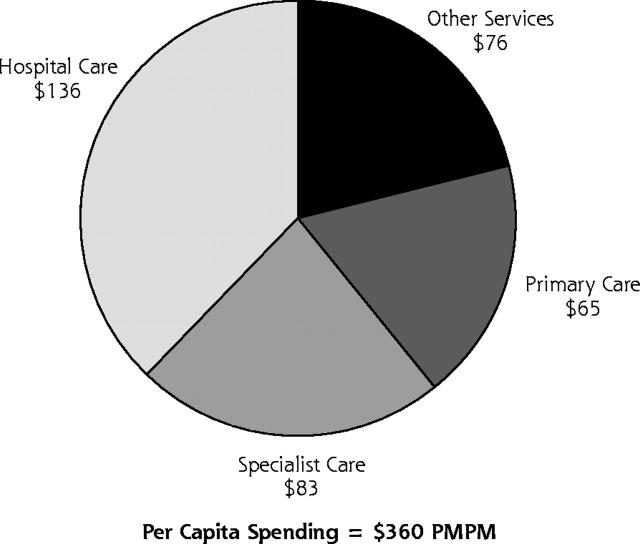
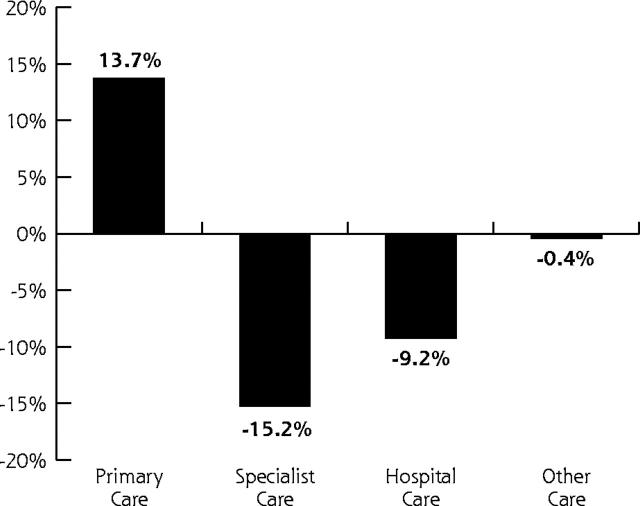
Results: The practice-level financial model suggests that full implementation of the New Model of care within the current fee-for-service system of reimbursement would result in a 26% increase in compensation (from 167,457 dollars to 210,288 dollars total annual compensation) for prototypical family physicians who maintain their current number of work hours. Alternatively, physicians could choose to decrease their work hours by 12% and maintain their current compensation. This result is sensitive to physician practice group size. The societal level financial model shows that modifications in the current reimbursement system could lead to further improvements in compensation for family physicians practicing the New Model of care. Reimbursement for e-visits and chronic disease management could further increase total annual compensation to 229,849 dollars for prototypical family physicians maintaining their current number of work hours. The widespread introduction of quality-based physician incentive bonus payments similar to some current programs that have been implemented on a limited basis could further increase total annual compensation up to 254,500 dollars. The adoption of a mixed reimbursement model, which would add an annual per-patient fee, a chronic care bonus, and an overall performance bonus to the current reimbursement system, could increase total annual compensation for the prototypical family physician continuing the current number of hours worked to as much as 277,800 dollars, a 66% increase above current compensation levels. The cost of transition to the New Model is estimated to range from 23,442 dollars to 90,650 dollars per physician, depending on the assumed magnitude of productivity loss associated with implementing an electronic health record. The financial impact of enhanced use of primary care on the costs of health care in the United States was estimated. If every American used a primary care physician as their usual source of care, health care costs would likely decrease by 5.6%, resulting in national savings of 67 billion dollars per year, with an improvement in the quality of the health care provided.
Conclusions: Family physicians could use New Model efficiency to increase compensation or to reduce work time. There are alternative reimbursement methodologies compatible with the New Model that would allow family physicians to share in the health care cost savings achieved as a result of effective and efficient delivery of care. The New Model of care should enhance health care while propelling the US system toward improved performance and results that are satisfying to patients, health care professionals, purchasers, and payers. The New Model needs to be implemented now. Given the recognized need for improvements in the US health care system in the areas of quality, safety, access and costs, there is no reason to delay.
Figures
References
-
- Green LA, Graham R, Bagley B, et al. Task Force 1. Report of the Task Force on Patient Expectations, Core Values, Reintegration, and the New Model of Family Medicine. Ann Fam Med. 2004;2:S33–S50. Available at: http://www.annfammed.org/cgi/content/full/2/suppl_1/S33.
-
- Bucholtz JR, Matheny SC, Pugno PA, et al. Task Force Report 2. Report of the Task Force on Medical Education. Ann Fam Med. 2004;2:S51–S64. Available at: http://www.annfammed.org/cgi/content/full/2/suppl_1/S51.
-
- Jones WA, Avant RF, Davis N, Saultz J, Lyons P. Task Force Report 3. Report of the Task Force on Continuous Personal, Professional, and Practice Development in Family Medicine. Ann Fam Med. 2004;2: S65–S74. Available at: http://www.annfammed.org/cgi/content/full/2/suppl_1/S65.
-
- Dickinson JC, Evans KL, Carter J, Burke K. Task Force Report 4. Report of the Task Force on Marketing and Communications. Ann Fam Med. 2004;2: S75–S87. Available at: http://www.annfammed.org/cgi/content/full/2/suppl_1/S75.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous