

MR venography in the pediatric patient
- PMID: 15661699
- PMCID: PMC7975049
MR venography in the pediatric patient
Abstract
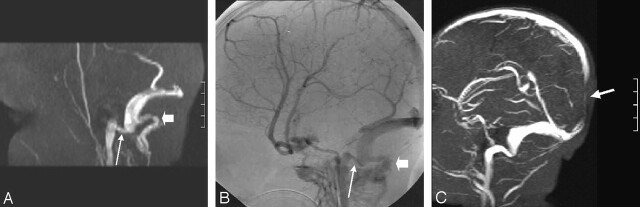
Background and purpose: Little is known about age-related changes in posterior fossa venous anatomy on 2D time-of-flight MR venography (MRV) or about artifacts that limit its accuracy in diagnosing venous occlusive disease. We evaluated pediatric appearances of posterior fossa venous drainage.
Methods: One hundred and eight children with normal MR imaging or minimal congenital anomalies underwent 2D MRV. Transverse sinus dominance and absence and the presence of an occipital sinus were correlated with age. Venous structure conspicuity was compared on source and maximum intensity projection images.
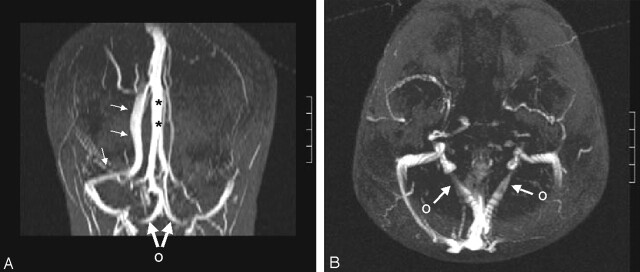
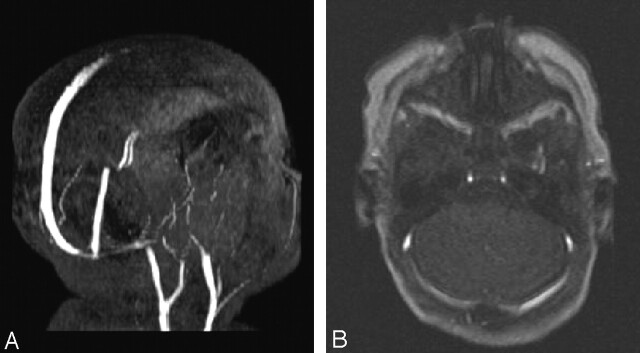
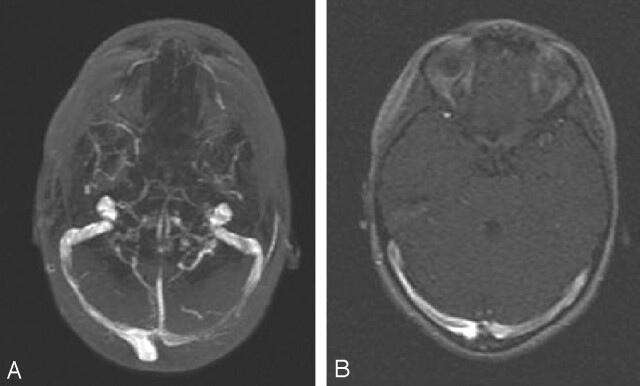
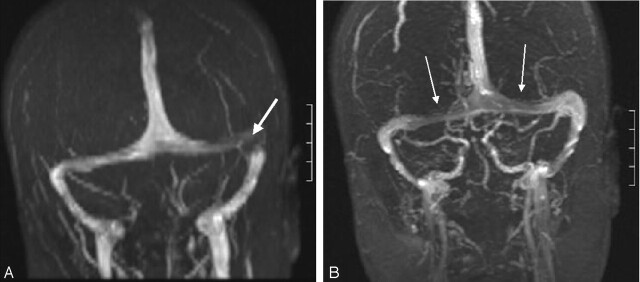
Results: Right, left, and codominance of the transverse sinus, respectively, was as follows: at < 25 months, 37%, 21%, and 42%; 25 months to 5 years, 35%, 30%, 35%; and > or =6 years, 50%, 16%, 34%. Transverse sinus dominance was not related to age between the three groups (P=.58, chi-square contingency), but some relationship was observed when patients <6 years were compared to those > or =6 years (P=.032). Chi-square trends showed a mildly positive correlation between age and an absent transverse sinus (P=.026) and a decreasing trend in the presence of an occipital sinus with age (P=.038). Saturation effects due to in-plane/slow flow were worse in patients <25 months; effects in the transverse sinuses or internal jugular veins were miminized with coronal or axial imaging, respectively.
Conclusion: 2D TOF MRV shows age-related changes in venous anatomy. Caution should be used before posterior fossa venous occlusive disease is diagnosed on the basis of signal intensity loss, especially in neonates and young infants.
Figures


Similar articles
-
2D time-of-flight MR venography in neonates: anatomy and pitfalls.AJNR Am J Neuroradiol. 2006 Oct;27(9):1913-8. AJNR Am J Neuroradiol. 2006. PMID: 17032865 Free PMC article.
-
Torcular Herophili classification and evaluation of dural venous sinus variations using digital subtraction angiography and magnetic resonance venographies.Surg Radiol Anat. 2014 Aug;36(6):527-36. doi: 10.1007/s00276-013-1223-0. Epub 2013 Oct 24. Surg Radiol Anat. 2014. PMID: 24154635
-
Transverse dural sinuses: incidence of anatomical variants and flow artefacts with 2D time-of-flight MR venography at 1 Tesla.Radiol Med. 2010 Mar;115(2):326-38. doi: 10.1007/s11547-010-0480-9. Epub 2010 Jan 8. Radiol Med. 2010. PMID: 20058094 English, Italian.
-
A review of extraaxial developmental venous anomalies of the brain involving dural venous flow or sinuses: persistent embryonic sinuses, sinus pericranii, venous varices or aneurysmal malformations, and enlarged emissary veins.Neurosurg Focus. 2018 Jul;45(1):E9. doi: 10.3171/2018.5.FOCUS18107. Neurosurg Focus. 2018. PMID: 29961384 Review.
-
Normal and variant anatomy of the dural venous sinuses.Semin Ultrasound CT MR. 1994 Dec;15(6):499-519. doi: 10.1016/s0887-2171(05)80019-8. Semin Ultrasound CT MR. 1994. PMID: 7880564 Review.
Cited by
-
Visualising the Dural Venous Sinuses Using Volume Tracing, a Novel Approach.Adv Exp Med Biol. 2023;1392:61-84. doi: 10.1007/978-3-031-13021-2_4. Adv Exp Med Biol. 2023. PMID: 36460846
-
Venous pathologies in paediatric neuroradiology: from foetal to adolescent life.Neuroradiology. 2020 Jan;62(1):15-37. doi: 10.1007/s00234-019-02294-x. Epub 2019 Nov 9. Neuroradiology. 2020. PMID: 31707531 Review.
-
Corpus callosotomy in children.Childs Nerv Syst. 2006 Aug;22(8):999-1011. doi: 10.1007/s00381-006-0133-4. Epub 2006 Jul 8. Childs Nerv Syst. 2006. PMID: 16830167 Clinical Trial.
-
External hydrocephalus in infants: six cases with MR venogram and flow quantification correlation.Childs Nerv Syst. 2011 Dec;27(12):2087-96. doi: 10.1007/s00381-011-1549-z. Epub 2011 Aug 11. Childs Nerv Syst. 2011. PMID: 21833725
-
Fate of the three embryonic dural sinuses in infants: the primitive tentorial sinus, occipital sinus, and falcine sinus.Neuroradiology. 2018 Mar;60(3):325-333. doi: 10.1007/s00234-018-1980-x. Epub 2018 Jan 22. Neuroradiology. 2018. PMID: 29356857
References
MeSH terms
LinkOut - more resources
Full Text Sources