

Accuracy of dynamic perfusion CT with deconvolution in detecting acute hemispheric stroke
- PMID: 15661711
- PMCID: PMC7975040
Accuracy of dynamic perfusion CT with deconvolution in detecting acute hemispheric stroke
Abstract
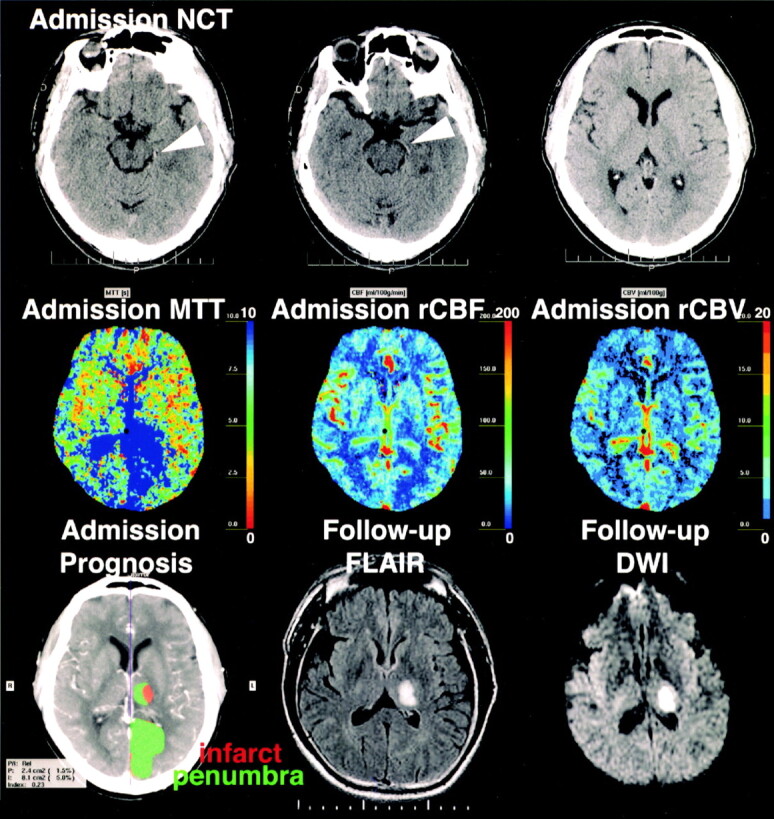
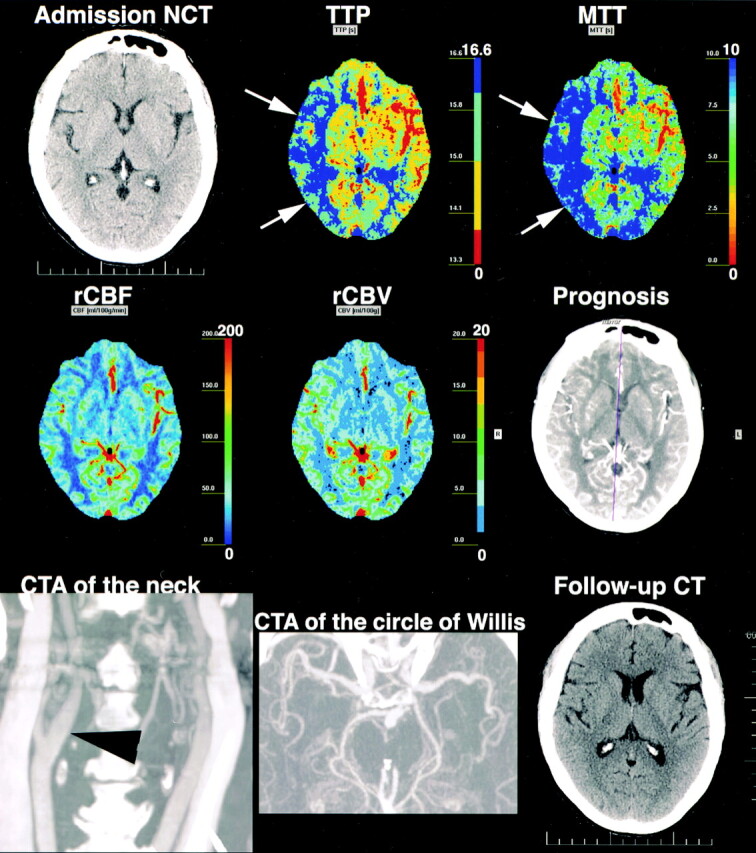
Background and purpose: Dynamic perfusion CT (PCT) with deconvolution produces maps of time-to-peak (TTP), mean transit time (MTT), regional cerebral blood flow (rCBF), and regional cerebral blood volume (rCBV), with a computerized automated map of the infarct and penumbra. We determined the accuracy of these maps in patients with suspected acute hemispheric stroke.
Methods: Forty-six patients underwent nonenhanced CT and dynamic PCT, with follow-up CT or MR imaging. Two observers reviewed the nonenhanced studies for signs of stroke and read the PCT maps for TTP, MTT, rCBF, and rCBV abnormalities. Sensitivity, specificity, accuracy, and interobserver agreement were compared (Wilcoxon tests). Nonenhanced CT and PCT data were reviewed for stroke extent according to previously reported methods. Sensitivity, specificity, and accuracy of the computerized maps in detecting ischemia and its extent were determined.
Results: Compared with nonenhanced CT, PCT maps were significantly more accurate in detecting stroke (75.7-86.0% vs. 66.2%; P <.01), MTT maps were significantly more sensitive (77.6% vs. 69.2%; P <.01), and rCBF and rCBV maps were significantly more specific (90.9% and 92.7%, respectively, vs. 65.0%; P <.01). Regarding stroke extent, PCT maps were significantly more sensitive than nonenhanced CT (up to 94.4% vs. 42.9%; P <.01) and had higher interobserver agreement (up to 0.763). For the computerized map, sensitivity, specificity, and accuracy, respectively, were 68.2%, 92.3%, and 88.1% in detecting ischemia and 72.2%, 91.8%, and 87.9% in showing the extent.
Conclusion: Dynamic PCT maps are more accurate than nonenhanced CT in detecting hemispheric strokes. Despite limited spatial coverage, PCT is highly reliable to assess the stroke extent.
Figures
Similar articles
-
Optimal brain perfusion CT coverage in patients with acute middle cerebral artery stroke.AJNR Am J Neuroradiol. 2010 Apr;31(4):691-5. doi: 10.3174/ajnr.A1880. Epub 2009 Nov 26. AJNR Am J Neuroradiol. 2010. PMID: 19942712 Free PMC article.
-
Perfusion CT in acute stroke: predictive value of perfusion parameters in assessing tissue viability versus infarction.Radiol Med. 2007 Feb;112(1):113-22. doi: 10.1007/s11547-007-0125-9. Epub 2007 Feb 22. Radiol Med. 2007. PMID: 17310286 English, Italian.
-
[Quantitative perfusion imaging by multi-slice CT in stroke patients].Rofo. 2003 Jun;175(6):806-13. doi: 10.1055/s-2003-39928. Rofo. 2003. PMID: 12811694 German.
-
Arterial spin-labeling in routine clinical practice, part 2: hypoperfusion patterns.AJNR Am J Neuroradiol. 2008 Aug;29(7):1235-41. doi: 10.3174/ajnr.A1033. Epub 2008 Mar 20. AJNR Am J Neuroradiol. 2008. PMID: 18356467 Free PMC article. Review.
-
Stroke imaging research road map.Neuroimaging Clin N Am. 2011 May;21(2):239-45, ix. doi: 10.1016/j.nic.2011.01.009. Epub 2011 Mar 15. Neuroimaging Clin N Am. 2011. PMID: 21640297 Free PMC article. Review.
Cited by
-
Acute stroke: a comparison of different CT perfusion algorithms and validation of ischaemic lesions by follow-up imaging.Eur Radiol. 2012 Dec;22(12):2559-67. doi: 10.1007/s00330-012-2529-8. Epub 2012 Jun 21. Eur Radiol. 2012. PMID: 22717727
-
Clinical outcome and imaging follow-up in acute stroke patients with normal perfusion CT and normal CT angiography.Neuroradiology. 2011 Feb;53(2):79-88. doi: 10.1007/s00234-010-0702-9. Epub 2010 Apr 27. Neuroradiology. 2011. PMID: 20422406
-
CT angiography and perfusion CT in cerebral vasospasm after subarachnoid hemorrhage.AJNR Am J Neuroradiol. 2007 Apr;28(4):750-8. AJNR Am J Neuroradiol. 2007. PMID: 17416833 Free PMC article.
-
Optic nerve sheath diameters in healthy adults measured by computer tomography.Int J Ophthalmol. 2015 Dec 18;8(6):1240-4. doi: 10.3980/j.issn.2222-3959.2015.06.30. eCollection 2015. Int J Ophthalmol. 2015. PMID: 26682181 Free PMC article.
-
Imaging recommendations for acute stroke and transient ischemic attack patients: A joint statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of NeuroInterventional Surgery.AJNR Am J Neuroradiol. 2013 Nov-Dec;34(11):E117-27. doi: 10.3174/ajnr.A3690. Epub 2013 Aug 1. AJNR Am J Neuroradiol. 2013. PMID: 23907247 Free PMC article.
References
-
- Latchaw RE, Yonas H, Hunter GJ, et al. Council on Cardiovascular Radiology of the American Heart Association: guidelines and recommendations for perfusion imaging in cerebral ischemia. Stroke 2003;34:1084–1104 - PubMed
-
- Lev MH, Segal AZ, Farkas J, et al. Utility of perfusion-weighted CT imaging in acute middle cerebral artery stroke treated with intra-arterial thrombolysis: prediction of final infarct volume and clinical outcome. Stroke 2001;32:2021–2027 - PubMed
-
- Hunter GJ, Silvennoinen HM, Hamberg LM, et al. Whole-brain CT perfusion measurement of perfused cerebral blood volume in acute ischemic stroke: probability curve for regional infarction. Radiology 2003;227:725–730 - PubMed
-
- Wintermark M, Bogousslavsky J. Imaging of acute ischemic brain injury: the return of computed tomography. Curr Opin Neurol 2003;16:59–63 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical