

The impact of Medicaid managed care on hospitalizations for ambulatory care sensitive conditions
- PMID: 15663700
- PMCID: PMC1361124
- DOI: 10.1111/j.1475-6773.2005.00340.x
The impact of Medicaid managed care on hospitalizations for ambulatory care sensitive conditions
Abstract
Objective: To determine whether Medicaid managed care is associated with lower hospitalization rates for ambulatory care sensitive conditions than Medicaid fee-for-service. We also explored whether there was a differential effect of Medicaid managed care by patient's race or ethnicity on the hospitalization rates for ambulatory care sensitive conditions.
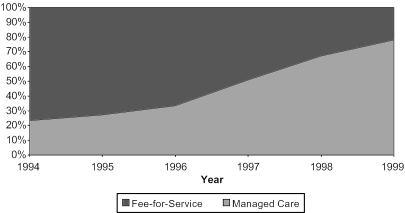
Data sources/study setting: Electronic hospital discharge abstracts for all California temporary assistance to needy families (TANF)-eligible Medicaid beneficiaries less than age 65 who were admitted to acute care hospitals in California between 1994 and 1999.
Study design: We performed a cross-sectional comparison of average monthly rates of admission for ambulatory care-sensitive conditions among TANF-eligible Medicaid beneficiaries in fee-for-service, voluntary managed care, and mandatory managed care.
Data collection/extraction methods: We calculated monthly rates of ambulatory care-sensitive condition admission rates by counting admissions for specified conditions in hospital discharge files and dividing the monthly count of admissions by the size of the at-risk population derived from a separate monthly Medicaid eligibility file. We used multivariate Poisson regression to model monthly hospital admission rates for ambulatory care-sensitive conditions as a function of the Medicaid delivery model controlling for admission month, admission year, patient age, sex, race/ethnicity, and county of residence.
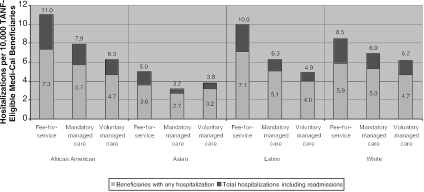
Principal findings: The adjusted average monthly hospitalization rate for ambulatory care-sensitive conditions per 10,000 was 9.36 in fee-for-service, 6.40 in mandatory managed care, and 5.25 in voluntary managed care (p<.0001 for all pairwise comparisons). The difference in hospitalization rates for ambulatory care sensitive conditions in Medicaid fee-for-service versus managed care was significantly larger for patients from minority groups than for whites.
Conclusions: Selection bias in voluntary Medicaid managed care programs exaggerates the differences between managed care and fee-for-service, but the 33 percent lower rate of hospitalizations for ambulatory care sensitive conditions found in mandatory managed care compared with fee-for-service suggests that Medicaid managed care is associated with a large reduction in hospital utilization, which likely reflects health benefits. The greater effect of Medicaid managed care for minority compared with white beneficiaries is consistent with other findings that suggest that managed care is associated with improvements in access to ambulatory care for those patients who have traditionally faced the greatest barriers to health care.
Figures
Similar articles
-
Impact of a Medicaid primary care provider and preventive care on pediatric hospitalization.Pediatrics. 1998 Mar;101(3):E1. doi: 10.1542/peds.101.3.e1. Pediatrics. 1998. PMID: 9481020
-
Medicaid re-enrollment policies and children's risk of hospitalizations for ambulatory care sensitive conditions.Med Care. 2008 Oct;46(10):1049-54. doi: 10.1097/MLR.0b013e318185ce24. Med Care. 2008. PMID: 18815526
-
Racial and ethnic differences in receipt of primary care services between medicaid fee-for-service and managed care plans.J Ambul Care Manage. 2007 Jul-Sep;30(3):264-73. doi: 10.1097/01.JAC.0000278986.18428.12. J Ambul Care Manage. 2007. PMID: 17581438
-
Managed care for children: effect on access to care and utilization of health services.Future Child. 1998 Summer-Fall;8(2):39-59. Future Child. 1998. PMID: 9782649 Review.
-
Medicaid managed care and children: an overview.Future Child. 1998 Summer-Fall;8(2):93-104. Future Child. 1998. PMID: 9782652 Review.
Cited by
-
Something is amiss in Denmark: a comparison of preventable hospitalisations and readmissions for chronic medical conditions in the Danish Healthcare system and Kaiser Permanente.BMC Health Serv Res. 2011 Dec 22;11:347. doi: 10.1186/1472-6963-11-347. BMC Health Serv Res. 2011. PMID: 22192270 Free PMC article.
-
Are smoking and alcohol misuse associated with subsequent hospitalizations for ambulatory care sensitive conditions?J Behav Health Serv Res. 2011 Jan;38(1):3-15. doi: 10.1007/s11414-010-9215-x. J Behav Health Serv Res. 2011. PMID: 20464519
-
Capitation and enhanced fee-for-service models for primary care reform: a population-based evaluation.CMAJ. 2009 May 26;180(11):E72-81. doi: 10.1503/cmaj.081316. CMAJ. 2009. PMID: 19468106 Free PMC article.
-
Impact of Statewide Mandatory Medicaid Managed Care (SMMC) Programs on Hospital Obstetric Outcomes.Healthcare (Basel). 2022 May 9;10(5):874. doi: 10.3390/healthcare10050874. Healthcare (Basel). 2022. PMID: 35628011 Free PMC article.
-
A common denominator: calculating hospitalization rates for ambulatory care-sensitive conditions in California.Prev Chronic Dis. 2011 Sep;8(5):A102. Epub 2011 Aug 15. Prev Chronic Dis. 2011. PMID: 21843405 Free PMC article.
References
-
- Agency for Health Research and Quality 2004 http://www.qualityindicators.ahrq.gov/data/hcup/prevqi.htm “Prevention Quality Indicators, Revision 3” Available at.
-
- Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L. “Impact of Socioeconomic Status on Hospital Use in New York City.”. Health Affairs. 1993;12(1):162–73. - PubMed
-
- Bindman A, Grumbach K, Osmond D, Komaromy M, Vranizan K, Lurie N, Billings J, Stewart A. “Preventable Hospitalizations and Access to Health Care.”. Journal of the American Medical Association. 1995;274(4):305–11. - PubMed
-
- Bindman A, Yoon J, Grumbach K. “Trends in Physician Participation in Medicaid: The California Experience.”. Journal of Ambulatory Care Management. 2003;26(4):334–43. - PubMed
-
- Coughlin T, Long S. “Effects of Medicaid Managed Care on Adults.”. Medical Care. 2000;38(4):433–46. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
