

Quetiapine augmentation of SRIs in treatment refractory obsessive-compulsive disorder: a double-blind, randomised, placebo-controlled study [ISRCTN83050762]
- PMID: 15667657
- PMCID: PMC547907
- DOI: 10.1186/1471-244X-5-5
Quetiapine augmentation of SRIs in treatment refractory obsessive-compulsive disorder: a double-blind, randomised, placebo-controlled study [ISRCTN83050762]
Abstract
Background: Although serotonin reuptake inhibitors are effective in the treatment of OCD, many patients fail to respond to these agents. Growing evidence from open-label and placebo-controlled trials suggests a role for augmentation of SRIs with atypical antipsychotics in OCD. Quetiapine is generally well tolerated and previous open-label data has produced mixed results in OCD and additional controlled data is needed.
Methods: We undertook a double-blind, randomised, parallel-group, flexible-dose, placebo-controlled study of quetiapine augmentation in subjects who had responded inadequately to open-label treatment with an SRI for 12 weeks. Following informed consent and screening, forty-two subjects were randomised to either placebo or quetiapine for six weeks.
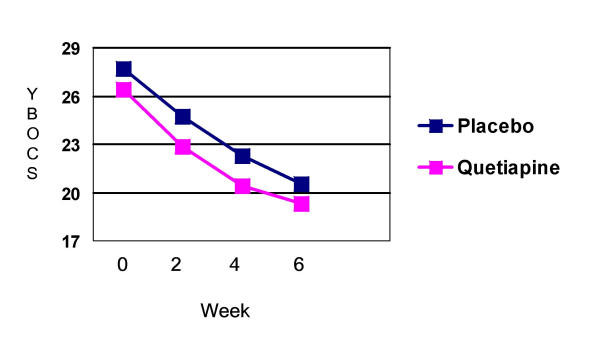
Results: There was significant improvement from baseline to endpoint on the Yale-Brown Obsessive-Compulsive Scale in both the quetiapine and placebo groups (quetiapine, n = 20, p < 0.0001; placebo, n = 21, p = 0.001) with 40% (n = 8) of quetiapine and 47.6% (n = 10) of placebo treated subjects being classified as responders. Quetiapine did not demonstrate a significant benefit over placebo at the end of the six-week treatment period (p = .636). Similarly quetiapine failed to separate from placebo in the subgroup of subjects (n = 10) with co-morbid tics. Quetiapine was generally well tolerated.
Conclusions: In this study, quetiapine augmentation was no more effective than placebo augmentation of SRIs. A number of limitations in study design make comparisons with previous studies in this area difficult and probably contributed to our negative findings. Future work in this important clinical area should address these limitations.
Figures
Similar articles
-
A double-blind, randomized, placebo-controlled trial of quetiapine addition in patients with obsessive-compulsive disorder refractory to serotonin reuptake inhibitors.J Clin Psychiatry. 2004 Aug;65(8):1040-8. doi: 10.4088/jcp.v65n0803. J Clin Psychiatry. 2004. PMID: 15323587 Clinical Trial.
-
Quetiapine augmentation in obsessive-compulsive disorder resistant to serotonin reuptake inhibitors: an open-label study.J Clin Psychiatry. 2005 Jan;66(1):73-9. doi: 10.4088/jcp.v66n0110. J Clin Psychiatry. 2005. PMID: 15669891 Clinical Trial.
-
Quetiapine addition to serotonin reuptake inhibitors in patients with severe obsessive-compulsive disorder: a double-blind, randomized, placebo-controlled study.J Clin Psychopharmacol. 2008 Oct;28(5):550-4. doi: 10.1097/JCP.0b013e318185e735. J Clin Psychopharmacol. 2008. PMID: 18794652 Clinical Trial.
-
A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder.Mol Psychiatry. 2006 Jul;11(7):622-32. doi: 10.1038/sj.mp.4001823. Epub 2006 Apr 4. Mol Psychiatry. 2006. PMID: 16585942
-
[Efficacy of antipsychotic augmentation therapy in treatment-resistant obsessive-compulsive disorder: a meta-analysis of double-blind, randomised, placebo-controlled trials].Fortschr Neurol Psychiatr. 2011 Aug;79(8):453-66. doi: 10.1055/s-0031-1273397. Epub 2011 Aug 1. Fortschr Neurol Psychiatr. 2011. PMID: 21809258 Review. German.
Cited by
-
Critical Review of the Use of Second-Generation Antipsychotics in Obsessive-Compulsive and Related Disorders.Drugs R D. 2018 Sep;18(3):167-189. doi: 10.1007/s40268-018-0246-8. Drugs R D. 2018. PMID: 30171515 Free PMC article. Review.
-
Catechol-O-Methyltransferase Gene Polymorphisms in Specific Obsessive-Compulsive Disorder Patients' Subgroups.J Mol Neurosci. 2016 Jan;58(1):129-36. doi: 10.1007/s12031-015-0697-0. Epub 2015 Dec 19. J Mol Neurosci. 2016. PMID: 26687156
-
Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders.BMC Psychiatry. 2014;14 Suppl 1(Suppl 1):S1. doi: 10.1186/1471-244X-14-S1-S1. Epub 2014 Jul 2. BMC Psychiatry. 2014. PMID: 25081580 Free PMC article. Review.
-
Should psychiatrists use atypical antipsychotics to treat nonpsychotic anxiety?Psychiatry (Edgmont). 2009 Jun;6(6):29-37. Psychiatry (Edgmont). 2009. PMID: 19724759 Free PMC article.
-
Second generation antipsychotic-induced obsessive-compulsive symptoms in schizophrenia: a review of the experimental literature.Curr Psychiatry Rep. 2014 Nov;16(11):510. doi: 10.1007/s11920-014-0510-8. Curr Psychiatry Rep. 2014. PMID: 25256097 Review.
References
-
- Murray CJL LAD. Global burden of disease: a comprehensive assessment of mortality from diseases injuries and risk factors in 1990 and projected to 2020. Harvard: WHO; 1996.
-
- Greist JH, Bandelow B, Hollander E, Marazziti D, Montgomery SA, Nutt DJ, Okasha A, Swinson RP, Zohar J. WCA recommendations for the long-term treatment of obsessive-compulsive disorder in adults. CNS Spectr. 2003;8:7–16. - PubMed
-
- Greist JH, Jefferson JW. Pharmacotherapy for obsessive-compulsive disorder. Br J Psychiatry Suppl. 1998:64–70. - PubMed
-
- Pigott TA, Seay SM. A review of the efficacy of selective serotonin reuptake inhibitors in obsessive-compulsive disorder. J Clin Psychiatry. 1999;60:101–106. - PubMed
-
- Saxena S, Wang D, Bystritsky A, Baxter LRJ. Risperidone augmentation of SRI treatment for refractory obsessive-compulsive disorder. J Clin Psychiatry. 1996;57:303–306. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
