

Adherence to maintenance-phase antidepressant medication as a function of patient beliefs about medication
- PMID: 15671187
- PMCID: PMC1466796
- DOI: 10.1370/afm.238
Adherence to maintenance-phase antidepressant medication as a function of patient beliefs about medication
Erratum in
- Ann Fam Med. 2005 Nov-Dec;3(6):558
Abstract
Purpose: This study aimed to identify the demographic, psychiatric, and attitudinal predictors of treatment adherence during the maintenance phase of antidepressant treatment, ie, after symptoms and regimen are stabilized.
Methods: We surveyed 81 primary care patients given maintenance antidepressant medications regarding general adherence, recent missed doses, depression and treatment features, medication beliefs (necessity, concerns, harmfulness, and overprescription), and other variables. Additional data were collected from medical and payer records.
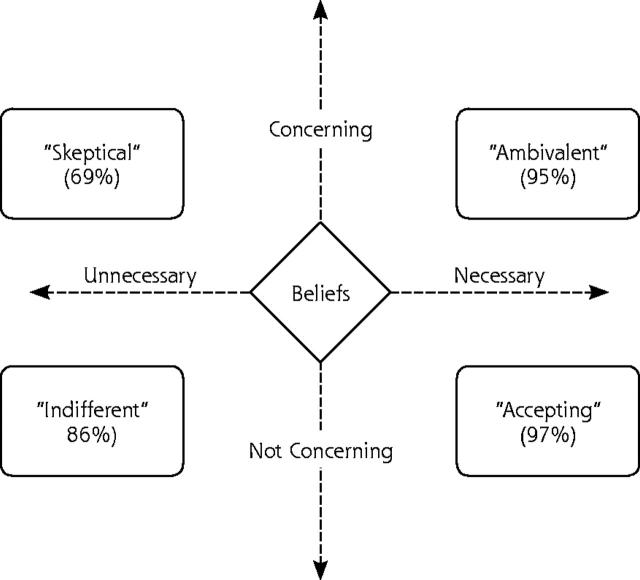
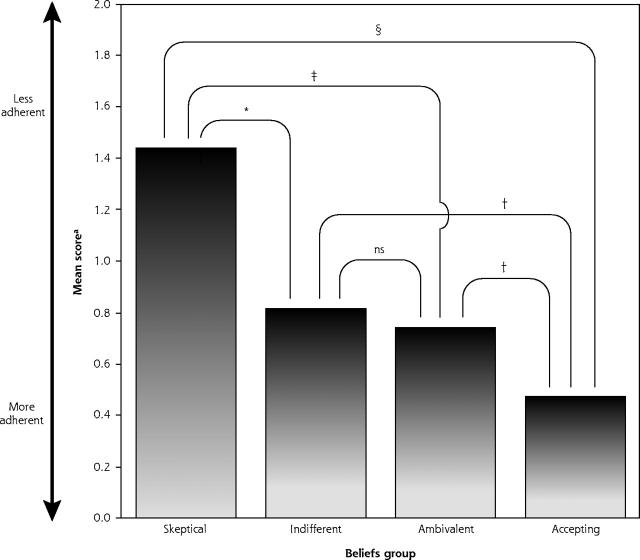
Results: Median treatment duration was 75 weeks. Adherence and beliefs were broadly dispersed and unrelated to treatment duration and type, physical functioning, and demographics. Multivariate analysis adjusting for social desirability, depression severity, and treatment duration indicated that an antidepressant-specific "necessity-minus-concerns" composite was strongly associated with both adherence outcomes. Specifically, adherence was highest when necessity exceeded concerns and lowest when concerns exceeded necessity. We crossed these 2 dimensions to characterize 4 patient attitudes toward antidepressants: skepticism, indifference, ambivalence, and acceptance.
Conclusions: Patients given maintenance antidepressants vary widely in adherence. This variation is primarily explained by the balance between their perceptions of need and harmfulness of antidepressant medication, in that adherence is lowest when perceived harm exceeds perceived need, and highest when perceived need exceeds perceived harm. We speculate on ways to tailor adherence strategies to patient beliefs. Subsequent research should determine whether patients' perceptions about medication predict depression outcomes, can be used to improve clinical management, and respond to behavioral intervention.
Figures
References
-
- Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER. The economic burden of depression in 1990. J Clin Psychiatr. 1993;54:405–418. - PubMed
-
- Wells KB, Stewart A, Hays RD, et al. The functioning and well-being of depressed patients: results from the medical outcomes study. J Am Med Assoc. 1989;262:914–919. - PubMed
-
- Depression Guideline Panel: Clinical Practice Guideline: Depression in primary Care, Vol. 2: Treatment of Major Depression (Clinical Practice Guideline No 5; AHCPR publ. No 93–0551). Rockville, MD; US Department of Health and Human Services, Public Health Services Agency of Health Care Policy Research; 1993.
-
- Regier DA, Hirschfeld RM, Goodwin FK, Burke JD Jr, Lazar JB, Judd LL. The NIMH depression awareness, recognition and treatment program: structure, aims, and scientific basis. Am J Psychiatry. 1988;145:1351–1357. - PubMed
-
- Maixner SM, Greden JF. Extended antidepressant maintenance and discontinuation syndromes. Depr Anx. 1998;8(Suppl 1):43–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical