

Exploration of DSM-IV criteria in primary care patients with medically unexplained symptoms
- PMID: 15673634
- PMCID: PMC1894627
- DOI: 10.1097/01.psy.0000149279.10978.3e
Exploration of DSM-IV criteria in primary care patients with medically unexplained symptoms
Abstract
Objectives: Investigators and clinicians almost always rely on Diagnostic and Statistical Manual of Mental Disorder, 4th edition's (DSM-IV) somatoform disorders (and its derivative diagnoses) to characterize and identify patients with medically unexplained symptoms (MUS). Our objective was to evaluate this use by determining the prevalence of DSM-IV somatoform and nonsomatoform disorders in patients with MUS proven by a gold standard chart review.
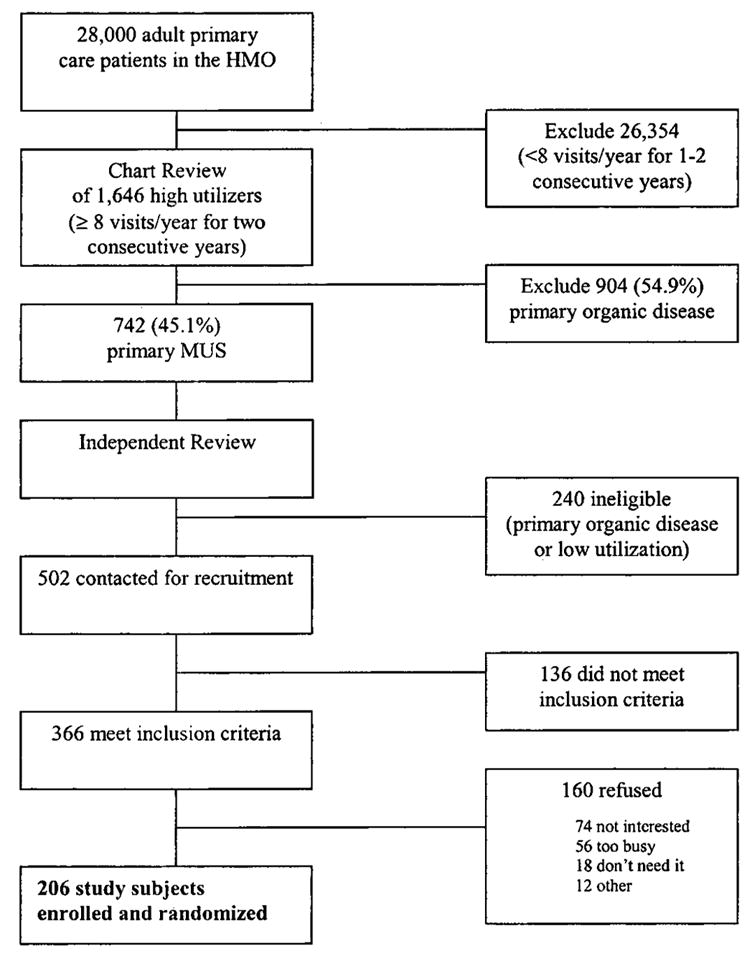
Methods: In a community-based staff model HMO, we identified subjects for a clinical trial using a systematic and reliable chart rating procedure among high-utilizing MUS patients. Only baseline data are reported here. The World Health Organization Composite International Diagnostic Interview provided full and abridged DSM-IV diagnoses. Patients with full or abridged DSM-IV somatoform diagnoses were labeled "DSM somatoform-positive," whereas those without them were labeled "DSM somatoform-negative."
Results: Two hundred six MUS patients averaged 13.6 visits in the year preceding study, 79.1% were females, and the average age was 47.7 years. We found that 124 patients (60.2%) had a nonsomatoform ("psychiatric") DSM-IV diagnosis of any type; 36 (17.5%) had 2 full nonsomatoform diagnoses, and 41 (19.9%) had >2; 92 (44.7%) had some full anxiety diagnosis and 94 (45.6%) had either full depression or minor depression diagnoses. However, only 9 of 206 (4.4%) had any full DSM-IV somatoform diagnosis, and only 39 (18.9%) had abridged somatization disorder. Thus, 48 (23.3%) were "DSM somatoform-positive" and 158 (76.7%) were "DSM somatoform-negative." The latter exhibited less anxiety, depression, mental dysfunction, and psychosomatic symptoms (all p <.001) and less physical dysfunction (p = .011). Correlates of this DSM somatoform-negative status were female gender (p = .007), less severe mental (p = .007), and physical dysfunction (p = .004), a decreased proportion of MUS (p <.10), and less psychiatric comorbidity (p <.10); c-statistic = 0.77.
Conclusion: We concluded that depression and anxiety characterized MUS patients better than the somatoform disorders. Our data suggested radically revising the somatoform disorders for DSM-V by incorporating a new, very large group of now-overlooked DSM somatoform-negative patients who were typically women with less severe dysfunction.
Figures
Similar articles
-
Depression, anxiety, and somatoform disorders: vague or distinct categories in primary care? Results from a large cross-sectional study.J Psychosom Res. 2009 Sep;67(3):189-97. doi: 10.1016/j.jpsychores.2009.04.013. Epub 2009 Jun 27. J Psychosom Res. 2009. PMID: 19686874 Clinical Trial.
-
Somatization revisited: diagnosis and perceived causes of common mental disorders.J Nerv Ment Dis. 2005 Feb;193(2):85-92. doi: 10.1097/01.nmd.0000152796.07788.b6. J Nerv Ment Dis. 2005. PMID: 15684910
-
A new, empirically established hypochondriasis diagnosis.Am J Psychiatry. 2004 Sep;161(9):1680-91. doi: 10.1176/appi.ajp.161.9.1680. Am J Psychiatry. 2004. PMID: 15337660
-
DSM-IV pain disorder in the general population. An exploration of the structure and threshold of medically unexplained pain symptoms.Eur Arch Psychiatry Clin Neurosci. 2006 Apr;256(3):187-96. doi: 10.1007/s00406-005-0625-3. Epub 2005 Nov 18. Eur Arch Psychiatry Clin Neurosci. 2006. PMID: 16328107 Review.
-
Somatoform disorders and medically unexplained symptoms in primary care.Dtsch Arztebl Int. 2015 Apr 17;112(16):279-87. doi: 10.3238/arztebl.2015.0279. Dtsch Arztebl Int. 2015. PMID: 25939319 Free PMC article. Review.
Cited by
-
Biomedical markers and psychiatric morbidity of neurasthenia spectrum disorders in four outpatient clinics in India.Indian J Psychiatry. 2008 Apr;50(2):87-95. doi: 10.4103/0019-5545.42394. Indian J Psychiatry. 2008. PMID: 19742222 Free PMC article.
-
Diagnostic concordance of neurasthenia spectrum disorders in Pune, India.Soc Psychiatry Psychiatr Epidemiol. 2007 Jul;42(7):561-72. doi: 10.1007/s00127-007-0196-x. Epub 2007 May 2. Soc Psychiatry Psychiatr Epidemiol. 2007. PMID: 17476439
-
Randomized effectiveness trial of an Internet, pure self-help, cognitive behavioral intervention for depressive symptoms in young adults.Cogn Behav Ther. 2009;38(4):222-34. doi: 10.1080/16506070802675353. Cogn Behav Ther. 2009. PMID: 19440896 Free PMC article. Clinical Trial.
-
Somatic symptoms in depression.Dialogues Clin Neurosci. 2006;8(2):227-39. doi: 10.31887/DCNS.2006.8.2/hpkapfhammer. Dialogues Clin Neurosci. 2006. PMID: 16889108 Free PMC article. Review.
-
Current debates over nosology of somatoform disorders.Ind Psychiatry J. 2012 Jan;21(1):4-10. doi: 10.4103/0972-6748.110939. Ind Psychiatry J. 2012. PMID: 23766571 Free PMC article.
References
-
- Escobar JI, Manu P, Matthews D, Lane T, Swartz M, Canino G. Medically unexplained physical symptoms, somatization disorder and abridged somatization: studies with the Diagnostic Interview Schedule. Psychiatric Development. 1989;3:235–45. - PubMed
-
- Escobar JI, Waitzkin H, Silver RC, Gara M, Holman A. Abridged somatization: a study in primary care. Psychosom Med. 1998;60:466–72. - PubMed
-
- Katon W, Russo J. Somatic symptoms and depression. J Fam Pract. 1989;29:65–9. - PubMed
-
- deGruy F, Crider J, Hashimi DK, Dickinson P, Mullins HC, Troncale J. Somatization disorder in a university hospital. J Fam Pract. 1987;25:579–84. - PubMed
-
- Smith RC, Gardiner JC, Lyles JS, Johnson M, Rost KM, Luo Z, Goddeeris J, Lein C, Given WE, Given B, Dwamena FC, Collins C, Van Egeren LF, Korban E, Kanj M, Haddad R. Minor acute illness: a preliminary research report of the ‘worried well’. J Fam Pract. 2002;51:24–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
