

Botulinum toxin type A therapy for hemifacial spasm
- PMID: 15674968
- PMCID: PMC6823221
- DOI: 10.1002/14651858.CD004899.pub2
Botulinum toxin type A therapy for hemifacial spasm
Update in
-
Botulinum toxin type A therapy for hemifacial spasm.Cochrane Database Syst Rev. 2020 Nov 19;11(11):CD004899. doi: 10.1002/14651858.CD004899.pub3. Cochrane Database Syst Rev. 2020. PMID: 33211908 Free PMC article.
Abstract
Background: Hemifacial spasm is characterised by unilateral involuntary contractions of muscles innervated by the facial nerve. The usual cause is a vessel touching the facial nerve near its origin from the brain stem. Although it is a benign condition it can cause significant cosmetic and functional disability. It is a chronic disease and spontaneous recovery is very rare. The two treatments routinely available are microvascular decompression and Botulinum Toxin type A (BtA) muscular injections.
Objectives: To determine whether botulinum toxin (BtA) is an effective and safe treatment for hemifacial spasm.
Search strategy: We searched the Cochrane Movement Disorders Group trials register, the Cochrane Central Register of Controlled Trials (The Cochrane Library Issue 1, 2004), MEDLINE (1977 to December 2003), EMBASE (1977 to December 2003), and reference lists of articles. We also contacted drug manufacturers and researchers in the field.
Selection criteria: Randomised studies comparing BtA with placebo in people with hemifacial spasm.
Data collection and analysis: Two reviewers independently assessed trial quality and extracted data. Study authors were contacted for additional information. Adverse effects information was collected from the trials.
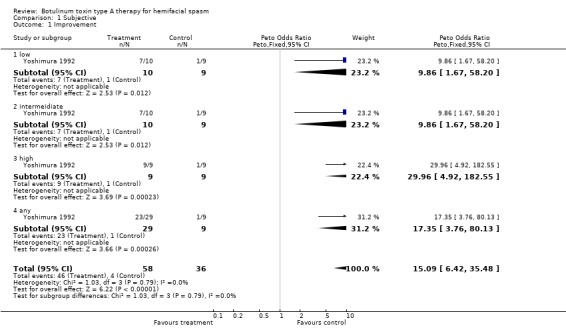
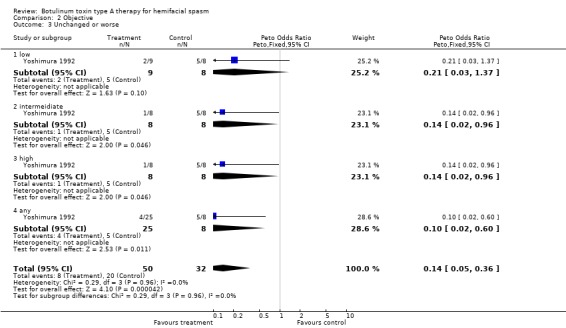
Main results: We found only one small randomised, placebo-controlled trial involving 11 people. It was a crossover trial during which patients underwent four sets of injections, comparing placebo with three different doses of BtA - formulation Botox(r) (low dose: one-half of the intermediate dose; intermediate dose; and high dose: twice the intermediate dose), and one of placebo. In this trial BtA was superior to placebo.
Authors' conclusions: The findings of this single eligible trial support the results of large, open, case-control studies showing a benefit rate between 76 and 100%. This effect size probably makes it very difficult to perform new large placebo controlled trials for hemifacial spasm. Despite the paucity of good quality controlled data, all the studies available suggest that BtA is effective and safe for treating hemifacial spasm. Future trials should explore technical factors such as the optimum treatment intervals, different injection techniques, doses, Bt types and formulations. Other issues include service delivery, quality of life, long-term efficacy, safety, and immunogenicity. BtA should be compared with surgical microvascular decompression.
Conflict of interest statement
Costa J, Ferreira JJ, Sampaio C, and Miguel C had been investigators in clinical trials sponsored by Elan, Allergan, and Ipsen. Ferreira JJ and Sampaio C were speakers in symposia promoted by Elan, Allergan, and Ipsen. Moore P has received fees from various companies marketing botulinum toxin for speaking at meetings and for advice. His unit has received funds for research.
Figures




Similar articles
-
Botulinum toxin type B for cervical dystonia.Cochrane Database Syst Rev. 2005 Jan 25;(1):CD004315. doi: 10.1002/14651858.CD004315.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2016 May 13;(5):CD004315. doi: 10.1002/14651858.CD004315.pub3. PMID: 15674941 Updated.
-
Botulinum toxin type A therapy for blepharospasm.Cochrane Database Syst Rev. 2005 Jan 25;(1):CD004900. doi: 10.1002/14651858.CD004900.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2020 Nov 19;11:CD004900. doi: 10.1002/14651858.CD004900.pub3. PMID: 15674969 Updated.
-
Botulinum toxin type A therapy for cervical dystonia.Cochrane Database Syst Rev. 2005 Jan 25;(1):CD003633. doi: 10.1002/14651858.CD003633.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2017 Dec 12;12:CD003633. doi: 10.1002/14651858.CD003633.pub3. PMID: 15674910 Updated.
-
Botulinum toxins for the prevention of migraine in adults.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD011616. doi: 10.1002/14651858.CD011616.pub2. Cochrane Database Syst Rev. 2018. PMID: 29939406 Free PMC article.
-
Botulinum toxin type A versus anticholinergics for cervical dystonia.Cochrane Database Syst Rev. 2005 Jan 25;2005(1):CD004312. doi: 10.1002/14651858.CD004312.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2021 Apr 14;4:CD004312. doi: 10.1002/14651858.CD004312.pub3. PMID: 15674939 Free PMC article. Updated.
Cited by
-
Clinical uses of botulinum neurotoxins: current indications, limitations and future developments.Toxins (Basel). 2012 Oct;4(10):913-39. doi: 10.3390/toxins4100913. Epub 2012 Oct 19. Toxins (Basel). 2012. PMID: 23162705 Free PMC article. Review.
-
"Contralateral Dry Eye in Hemifacial Spasm:" A New Clinical Sign.Asian J Neurosurg. 2019 Jul-Sep;14(3):996-998. doi: 10.4103/ajns.AJNS_48_19. Asian J Neurosurg. 2019. PMID: 31497150 Free PMC article.
-
Long-term adherence and response to botulinum toxin in different indications.Ann Clin Transl Neurol. 2021 Jan;8(1):15-28. doi: 10.1002/acn3.51225. Epub 2020 Dec 1. Ann Clin Transl Neurol. 2021. PMID: 33259153 Free PMC article.
-
Use of botulinum toxin A in adult neurological disorders: efficacy, tolerability and safety.CNS Drugs. 2008;22(9):725-38. doi: 10.2165/00023210-200822090-00002. CNS Drugs. 2008. PMID: 18698873 Review.
-
Health-related quality of life outcomes from botulinum toxin treatment in hemifacial spasm.Ther Adv Neurol Disord. 2017 Apr;10(4):211-216. doi: 10.1177/1756285616682676. Epub 2017 Feb 1. Ther Adv Neurol Disord. 2017. PMID: 28507604 Free PMC article.
References
References to studies included in this review
-
- Yoshimura DM, Aminoff MJ, Tami TA. Botulinum toxin therapy for Hemifacial Spasm. Neurology 1990;40 Suppl 1:381(974S).
- Yoshimura DM, Aminoff MJ, Tami TA, Scott AB. Treatment of Hemifacial Spasm with botulinum toxin. Muscle Nerve 1992;15:1045‐9. - PubMed
References to studies excluded from this review
-
- Mezaki T, Kaji R, Kimura J, Ogawa N. Treatment of Hemifacial Spasm with Type A Botulinum Toxin (AGN 191622): A Dose Finding Study and the Evaluation of Clinical Effect with Electromyography. No To Shinkei 1999;51:427‐32. - PubMed
-
- Price J, Farish S, Taylor H, O'Day J. Blepharospasm and Hemifacial Spasm. Randomized trial to determine the most appropriate location for botulinum toxin injections. Ophthalmology 1997;104(5):865‐8. - PubMed
-
- Sampaio C, Ferreira JJ, Simoes F, Rosas MJ, Magalhaes M, Correia AP, et al. DYSBOT: a single‐blind, randomized parallel study to determine whether any differences can be detected in the efficacy and tolerability of two formulations of botulinum toxin type A‐‐Dysport and Botox‐‐assuming a ratio of 4:1. Movement Disorders 1997;12(6):1013‐8. - PubMed
- Sampaio C, Ferreira JJ, Simões F, Rosas MJ, Magalhães M, Martins R, Bastos‐Lima A, Castro‐Caldas A. Dysbot: a single blind, randomized clinical trial to compare two different formulations of botulinum toxin type A. Movement Disorders 1995;10(3):387. - PubMed
Additional references
-
- Auger RG, Whisnant JP. Hemifacial spasm in Rochester and Olmsted County, Minnesota, 1960 to 1984. Archives of Neurology 1990;47(11):1233‐4. - PubMed
-
- Barker FG, Jannetta PJ, Bissonette DJ, Shields PT, Larkins MV, Jho HD. Microvascular decompression for hemifacial spasm. Journal of Neurosurgery 1995;82:201‐10. - PubMed
-
- Bernardi B, Zimmerman RA, Savino PJ, Adler C. Magnetic resonance tomographic angiography in the investigation of hemifacial spasm. Neuroradiology 1993;35(8):606‐11. - PubMed
-
- Brin. Scientific and Therapeutic Aspects of Botulinum Toxin. Philadelphia: Lippincott Williams & Wilkins, 2002.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical