

Recovery of the high-acceleration vestibulo-ocular reflex after vestibular neuritis
- PMID: 15675005
- PMCID: PMC2504572
- DOI: 10.1007/s10162-004-4035-4
Recovery of the high-acceleration vestibulo-ocular reflex after vestibular neuritis
Abstract
Vestibular neuritis (VN) usually leads to a sudden gain asymmetry of the high-acceleration horizontal vestibulo-ocular reflex (VOR). We asked whether this asymmetry decreases over time indicating peripheral recovery and/or central compensation. The horizontal VOR during rapid rotational head impulses to both sides was recorded with search coils in 37 patients at different time periods (1-240 weeks) after the onset of VN. In ten patients, sequential measurements were performed. Gains of the VOR during head impulses toward the ipsilesional side significantly increased after the initial drop (average gains: < 1 week: 0.35; 1-4 weeks: 0.33; 4-40 weeks: 0.55; 40-240 weeks: 0.50). Gains on the contralesional side, however, were only slightly reduced and showed no significant change. We conclude that, in contrast to patients after hemilabyrinthectomy or unilateral vestibular neurectomy, the ocular response to ipsilesional rotations in patients after VN improves over time. This finding suggests that ipsilesional recovery is peripheral or, if central, depends on spared peripheral function. The physiology of linear and nonlinear VOR pathways predicts a considerable gain reduction for contralesional head impulses if central compensation mechanisms are not engaged. Thus, the relatively preserved gain on the contralesional side can be explained only by central "upregulation". Apparently, for high accelerations of the head, effective central compensation after VN does not aim to balance the gains of the VOR but tries to boost the contralesional gain close to normal.
Figures
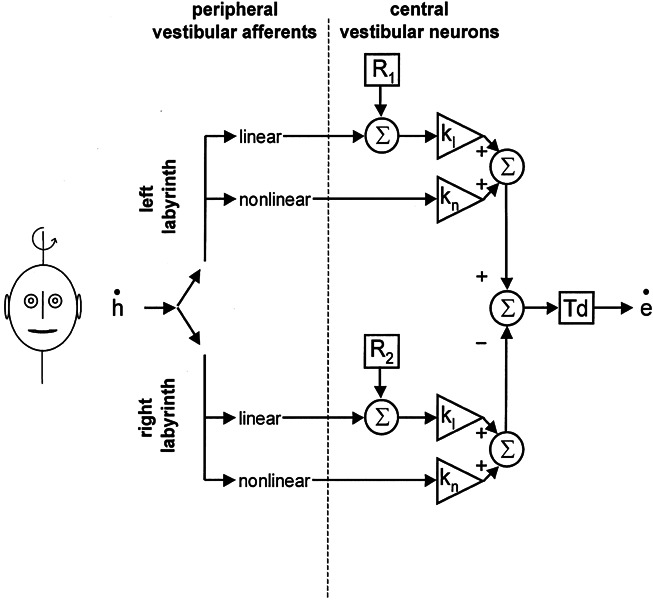
 ). This signal is
passed through linear and nonlinear pathways. kl and kn represent the corresponding central
gain elements of these two pathways. R
denotes the resting rate of central vestibular neurons, which is added to
the linear pathway. Td: time delay of the reflex (set to 7 ms in our
simulations).
). This signal is
passed through linear and nonlinear pathways. kl and kn represent the corresponding central
gain elements of these two pathways. R
denotes the resting rate of central vestibular neurons, which is added to
the linear pathway. Td: time delay of the reflex (set to 7 ms in our
simulations).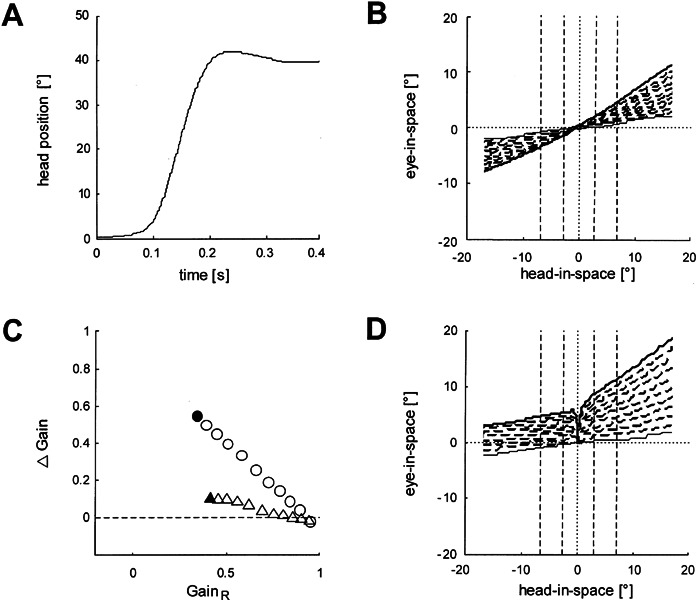
References
-
- Allum JH, Ledin T. Recovery of vestibulo-ocular reflex-function in subjects with an acute unilateral peripheral vestibular deficit. J. Vestib. Res. 1999;9:135–144. - PubMed
-
- Arbusow V, Schulz P, Strupp M, Dieterich M, von. Reinhardstoettner A, Rauch E, Brandt T. Distribution of herpes simplex virus type 1 in human geniculate and vestibular ganglia: implications for vestibular neuritis. Ann. Neurol. 1999;46:416–419. doi: 10.1002/1531-8249(199909)46:3<416::AID-ANA20>3.0.CO;2-W. - DOI - PubMed
-
- Arbusow V, Strupp M, Wasicky R, Horn AK, Schulz P, Brandt T. Detection of herpes simplex virus type 1 in human vestibular nuclei. Neurology. 2000;55:880–882. - PubMed
-
- Aw ST, Halmagyi GM, Haslwanter T, Curthoys IS, Yavor RA, Todd MJ. Three-dimensional vector analysis of the human vestibuloocular reflex in response to high-acceleration head rotations. II. responses in subjects with unilateral vestibular loss and selective semicircular canal occlusion. J. Neurophysiol. 1996;76:4021–4030. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
