

Comparing the clinical effectiveness of different new-born hearing screening strategies. A decision analysis
- PMID: 15679901
- PMCID: PMC549034
- DOI: 10.1186/1471-2458-5-12
Comparing the clinical effectiveness of different new-born hearing screening strategies. A decision analysis
Abstract
Background: Children with congenital hearing impairment benefit from early detection and treatment. At present, no model exists which explicitly quantifies the effectiveness of universal newborn hearing screening (UNHS) versus other programme alternatives in terms of early diagnosis. It has yet to be considered whether early diagnosis (within the first few months) of hearing impairment is of importance with regard to the further development of the child compared with effects resulting from a later diagnosis. The objective was to systematically compare two screening strategies for the early detection of new-born hearing disorders, UNHS and risk factor screening, with no systematic screening regarding their influence on early diagnosis.
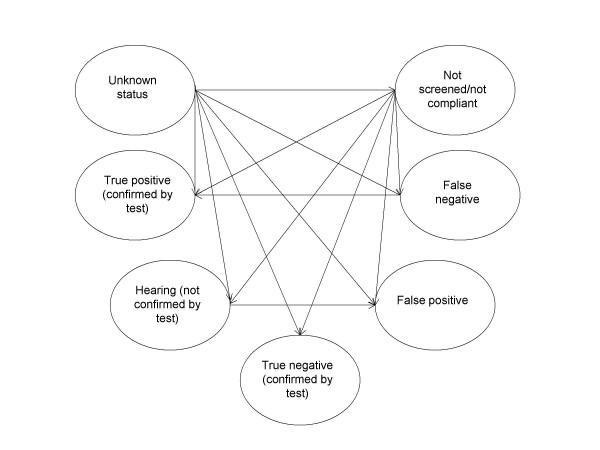
Design: Clinical effectiveness analysis using a Markov Model.
Data sources: Systematic literature review, empirical data survey, and expert opinion.
Target population: All newborn babies. TIME SCALE: 6, 12 and 120 months.
Perspective: Health care system. COMPARED STRATEGIES: UNHS, Risk factor screening (RS), no systematic screening (NS).
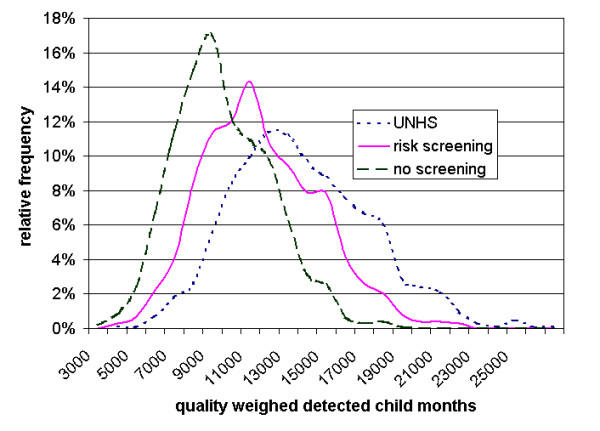
Outcome measures: Quality weighted detected child months (QCM).
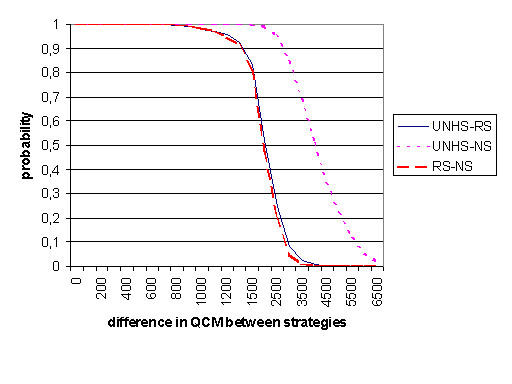
Results: UNHS detected 644 QCM up until the age of 6 months (72,2%). RS detected 393 child months (44,1%) and no systematic screening 152 child months (17,0%). UNHS detected 74,3% and 86,7% weighted child months at 12 and 120 months, RS 48,4% and 73,3%, NS 23,7% and 60,6%. At the age of 6 months UNHS identified approximately 75% of all children born with hearing impairment, RS 50% and NS 25%. At the time of screening UNHS marked 10% of screened healthy children for further testing (false positives), RS 2%. UNHS demonstrated higher effectiveness even under a wide range of relevant parameters. The model was insensitive to test parameters within the assumed range but results varied along the prevalence of hearing impairment.
Conclusion: We have shown that UNHS is able to detect hearing impairment at an earlier age and more accurately than selective RS. Further research should be carried out to establish the effects of hearing loss on the quality of life of an individual, its influence on school performance and career achievement and the differences made by early fitting of a hearing aid on these factors.
Figures
References
-
- Fortnum H, Davis A. Epidemiology of permanent childhood hearing impairment in Trent Region. 1985–1993. Br J Audiol. 1997;31:409–446. - PubMed
-
- Parving A, Hauch AM. Permanent childhood hearing impairment – some cross-sectional characteristics from a surveillance program. International Pediatrics. 2001;16:1–5.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
