

Autoantibodies and autoantigens in autoimmune hepatitis: important tools in clinical practice and to study pathogenesis of the disease
- PMID: 15679907
- PMCID: PMC544946
- DOI: 10.1186/1740-2557-1-2
Autoantibodies and autoantigens in autoimmune hepatitis: important tools in clinical practice and to study pathogenesis of the disease
Abstract
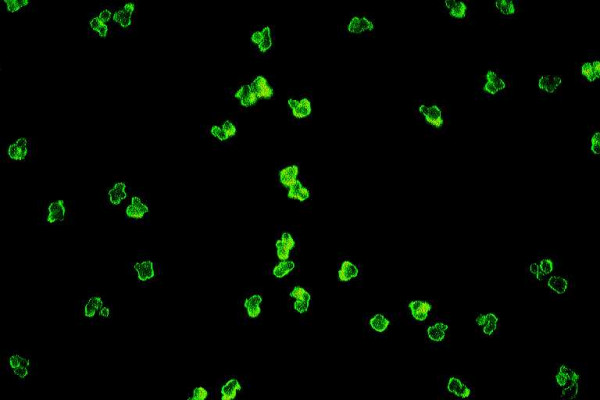
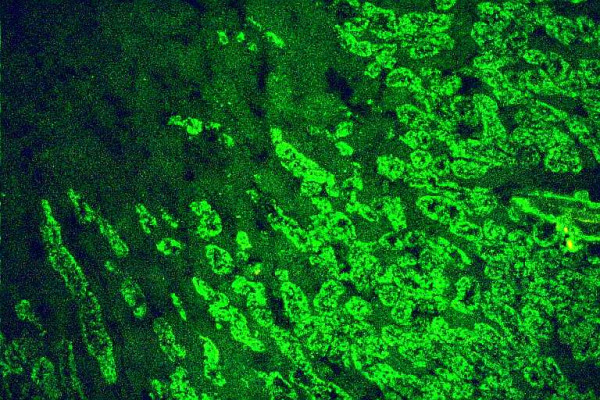
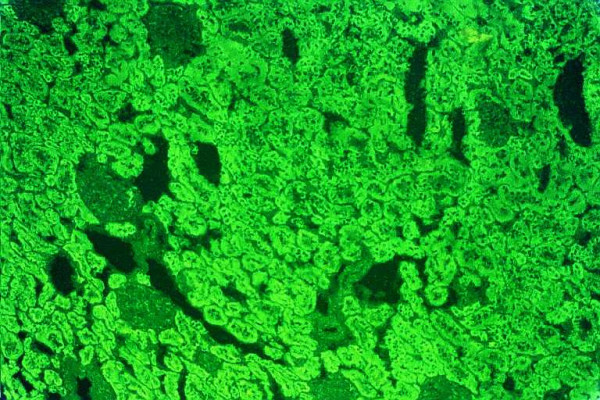
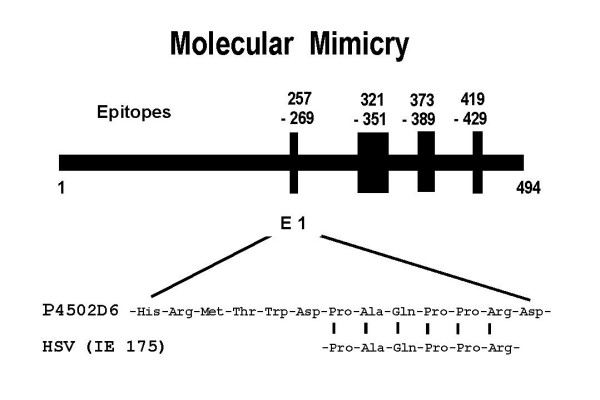
Autoimmune hepatitis (AIH) is a chronic necroinflammatory disease of the liver characterized by hypergammaglobulinemia, characteristic autoantibodies, association with HLA DR3 or DR4 and a favorable response to immunosuppressive treatment. The etiology is unknown. The detection of non-organ and liver-related autoantibodies remains the hallmark for the diagnosis of the disease in the absence of viral, metabolic, genetic, and toxic etiology of chronic hepatitis or hepatic injury. The current classification of AIH and the several autoantibodies/target-autoantigens found in this disease are reported. Current aspects on the significance of these markers in the differential diagnosis and the study of pathogenesis of AIH are also stated. AIH is subdivided into two major types; AIH type 1 (AIH-1) and type 2 (AIH-2). AIH-1 is characterized by the detection of smooth muscle autoantibodies (SMA) and/or antinuclear antibodies (ANA). Determination of antineutrophil cytoplasmic autoantibodies (ANCA), antibodies against the asialoglycoprotein receptor (anti-ASGP-R) and antibodies against to soluble liver antigens or liver-pancreas (anti-SLA/LP) may be useful for the identification of patients who are seronegative for ANA/SMA. AIH-2 is characterized by the presence of specific autoantibodies against liver and kidney microsomal antigens (anti-LKM type 1 or infrequently anti-LKM type 3) and/or autoantibodies against liver cytosol 1 antigen (anti-LC1). Anti-LKM-1 and anti-LKM-3 autoantibodies are also detected in some patients with chronic hepatitis C (HCV) and chronic hepatitis D (HDV). Cytochrome P450 2D6 (CYP2D6) has been documented as the major target-autoantigen of anti-LKM-1 autoantibodies in both AIH-2 and HCV infection. Recent convincing data demonstrated the expression of CYP2D6 on the surface of hepatocytes suggesting a pathogenetic role of anti-LKM-1 autoantibodies for the liver damage. Family 1 of UDP-glycuronosyltransferases has been identified as the target-autoantigen of anti-LKM-3. For these reasons the distinction between AIH and chronic viral hepatitis (especially of HCV) is of particular importance. Recently, the molecular target of anti-SLA/LP and anti-LC1 autoantibodies were identified as a 50 kDa UGA-suppressor tRNA-associated protein and a liver specific enzyme, the formiminotransferase cyclodeaminase, respectively. Anti-ASGP-R and anti-LC1 autoantibodies appear to correlate closely with disease severity and response to treatment suggesting a pathogenetic role of these autoantibodies for the hepatocellular injury. In general however, autoantibodies should not be used to monitor treatment, predict AIH activity or outcome. Finally, the current aspects on a specific form of AIH that may develop in some patients with a rare genetic syndrome, the autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome (APECED) are also given. Autoantibodies against liver microsomes (anti-LM) are the specific autoantibodies detected in AIH as a disease component of APECED but also in cases of dihydralazine-induced hepatitis. Cytochrome P450 1A2 has been identified as the target-autoantigen of anti-LM autoantibodies in both APECED-related AIH and dihydralazine-induced hepatitis. The latter may indicate that similar autoimmune pathogenetic mechanisms can lead to liver injury in susceptible individuals irrespective of the primary defect. Characterization of the autoantigen-autoantibody repertoire continues to be an attractive and important tool to get access to the correct diagnosis and to gain insight into the as yet unresolved mystery of how hepatic tolerance is given up and AIH ensues.
Figures
Similar articles
-
Autoantibodies and defined target autoantigens in autoimmune hepatitis: an overview.Eur J Intern Med. 2002 Aug;13(5):293-303. doi: 10.1016/s0953-6205(02)00089-4. Eur J Intern Med. 2002. PMID: 12144908
-
Cytochromes P450 and uridine triphosphate-glucuronosyltransferases: model autoantigens to study drug-induced, virus-induced, and autoimmune liver disease.Hepatology. 1997 Oct;26(4):1054-66. doi: 10.1002/hep.510260438. Hepatology. 1997. PMID: 9328334 Review.
-
[Autoimmune hepatitis and overlap syndrome: diagnosis].Praxis (Bern 1994). 2002 Aug 21;91(34):1339-46. doi: 10.1024/0369-8394.91.34.1339. Praxis (Bern 1994). 2002. PMID: 12233264 Review. German.
-
Autoantibodies against CYP2D6 and other drug-metabolizing enzymes in autoimmune hepatitis type 2.Drug Metab Rev. 2005;37(1):235-52. doi: 10.1081/dmr-200028798. Drug Metab Rev. 2005. PMID: 15747502 Review.
-
Autoimmune hepatitis.J Hepatol. 2000;32(1 Suppl):181-97. doi: 10.1016/s0168-8278(00)80425-0. J Hepatol. 2000. PMID: 10728804 Review.
Cited by
-
Pathogenic and Protective Autoantibodies in Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy (APECED).Antibodies (Basel). 2017 Jan 17;6(1):1. doi: 10.3390/antib6010001. Antibodies (Basel). 2017. PMID: 31548517 Free PMC article. Review.
-
Two of Them Do It Better: Novel Serum Biomarkers Improve Autoimmune Hepatitis Diagnosis.PLoS One. 2015 Sep 16;10(9):e0137927. doi: 10.1371/journal.pone.0137927. eCollection 2015. PLoS One. 2015. PMID: 26375394 Free PMC article.
-
Evaluation of classical and novel autoantibodies for the diagnosis of Primary Biliary Cholangitis-Autoimmune Hepatitis Overlap Syndrome (PBC-AIH OS).PLoS One. 2018 Mar 19;13(3):e0193960. doi: 10.1371/journal.pone.0193960. eCollection 2018. PLoS One. 2018. PMID: 29554146 Free PMC article.
-
The Contribution of B Cells in Autoimmune Liver Diseases.Semin Liver Dis. 2019 Nov;39(4):422-431. doi: 10.1055/s-0039-1688751. Epub 2019 Jun 21. Semin Liver Dis. 2019. PMID: 31226726 Free PMC article. Review.
-
The revised international autoimmune hepatitis score in chronic liver diseases including autoimmune hepatitis/overlap syndromes and autoimmune hepatitis with concurrent other liver disorders.J Autoimmune Dis. 2007 Jun 29;4:3. doi: 10.1186/1740-2557-4-3. J Autoimmune Dis. 2007. PMID: 17603886 Free PMC article.
References
-
- Berdal JE, Ebbesen J, Rydning A. Incidence and prevalence of autoimmune liver diseases. Tidsskr Nor Laegeforen. 1998;118:4517–4519. - PubMed
-
- Boberg KM, Aadland E, Jahnsen J, Raknerud N, Stiris M, Bell H. Incidence and prevalence of primary biliary cirrhosis, primary sclerosing cholangitis, and autoimmune hepatitis in a Norwegian population. Scand J Gastroenterol. 1998;33:99–103. - PubMed
-
- Manns MP, Strassburg CP. Autoimmune hepatitis: clinical challenges. Gastroenterology. 2001;120:1502–1517. - PubMed
-
- Czaja AJ. Drug therapy in the management of type 1 autoimmune hepatitis. Drugs. 1999;57:49–68. - PubMed
-
- Obermayer-Straub P, Strassburg CP, Manns MP. Autoimmune hepatitis. J Hepatol. 2000;32:181–197. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
