

The impact of implantable cardioverter-defibrillator therapy on survival in autosomal-dominant arrhythmogenic right ventricular cardiomyopathy (ARVD5)
- PMID: 15680719
- PMCID: PMC3133766
- DOI: 10.1016/j.jacc.2004.08.068
The impact of implantable cardioverter-defibrillator therapy on survival in autosomal-dominant arrhythmogenic right ventricular cardiomyopathy (ARVD5)
Abstract
Objectives: We sought to determine the impact of implantable cardioverter-defibrillator (ICD) therapy in patients with familial arrhythmogenic right ventricular cardiomyopathy (ARVC).
Background: Arrhythmogenic right ventricular cardiomyopathy is a cause of sudden cardiac death, which may be prevented by ICD.
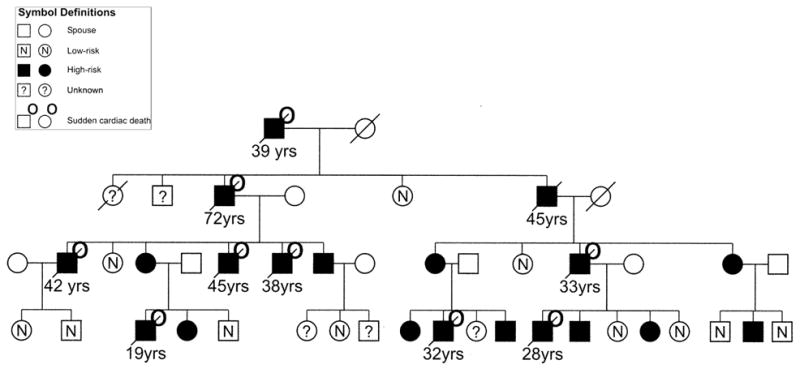
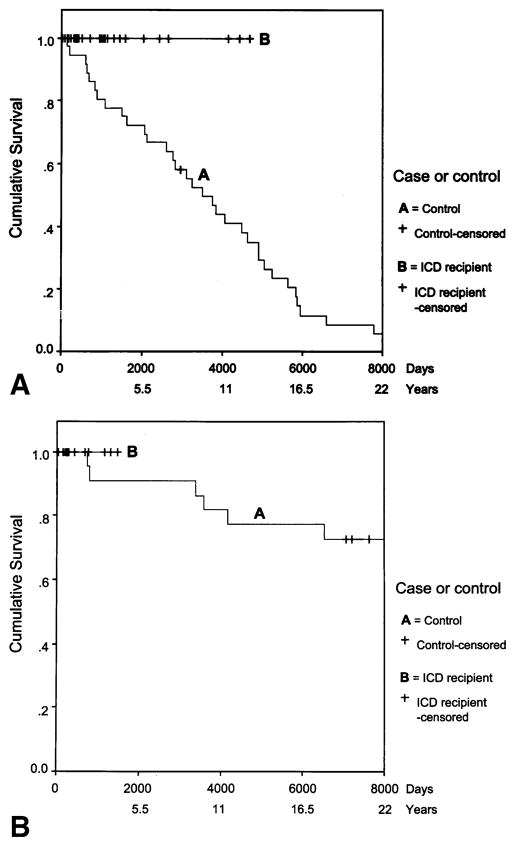
Methods: We studied 11 families in which a 3p25 deoxyribonucleic acid (DNA) haplotype at locus ARVD5 segregated with disease and compared mortality in subjects who received an ICD with that in control subjects who were matched for age, gender, ARVC status, and family. Subjects (n = 367) at 50% a priori risk of inheriting ARVC were classified as high risk (HR) (n = 197), low risk (n = 92), or unknown (n = 78) on the basis of clinical events, DNA haplotyping, and/or pedigree position. Forty-eight HR subjects (30 males, [median age 32 years] and 18 females [median age 41 years]) were followed after ICD (secondary to ventricular tachycardia [VT] in 27%). Survival was compared with 58 HR control subjects who were alive at the same age to-the-day at which the ICD subject received the device.
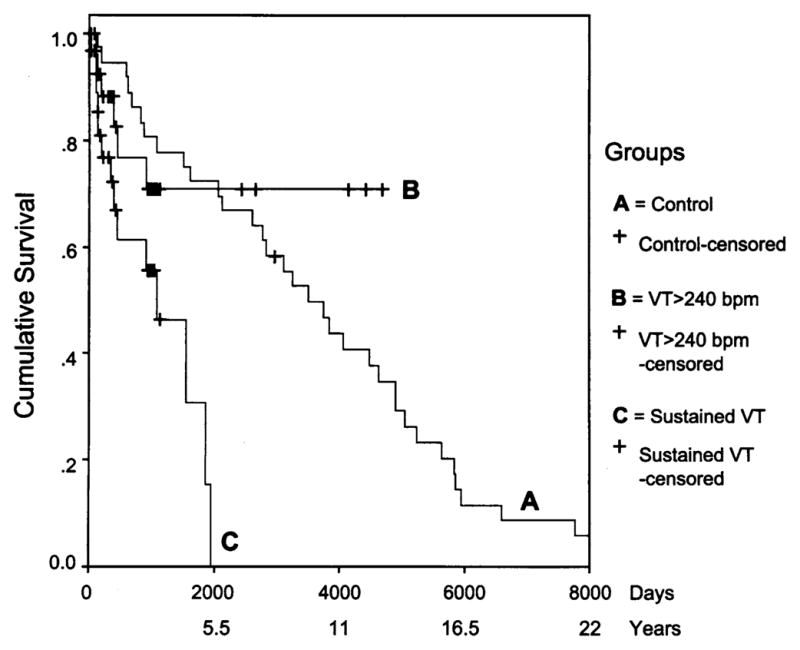
Results: In the HR group, 50% of males were dead by 39 years and females by 71 years: relative risk of death was 5.1 (95% confidence interval 3 to 8.5) for males. The five-year mortality rate after ICD in males was zero compared with 28% in control subjects (p = 0.009). Within five years, the ICD fired for VT in 70% and for VT >240 beats/min in 30%, with no difference in discharge rate when analyzed by ICD indication.
Conclusions: The unknown mutation at the ARVD5 locus causing ARVC results in high mortality. Risk stratification using genetic haplotyping and ICD therapy produced improved survival for males.
Figures

Comment in
-
Implantable cardioverter-defibrillator therapy in arrhythmogenic right ventricular cardiomyopathy: a role for genotyping in decision-making?J Am Coll Cardiol. 2005 Feb 1;45(3):409-11. doi: 10.1016/j.jacc.2004.11.009. J Am Coll Cardiol. 2005. PMID: 15680720 No abstract available.
References
-
- Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999;341:1882–90. - PubMed
-
- The Antiarrhythmics Versus Implantable Defibrillators (AVID) investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337:1576–84. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–40. - PubMed
-
- Connolly SJ, Gent M, Roberts RS, et al. Canadian Implantable Defibrillator Study (CIDS): a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation. 2000;101:1297–302. - PubMed
-
- Echt D, Liebson P, Mitchell L, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324:781–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
