

Economic evaluation of sirolimus-eluting stents
- PMID: 15684117
- PMCID: PMC545758
- DOI: 10.1503/cmaj.1041062
Economic evaluation of sirolimus-eluting stents
Abstract
Background: Sirolimus-eluting stents have recently been shown to reduce the risk of restenosis among patients who undergo percutaneous coronary intervention (PCI). Given that sirolimus-eluting stents cost about 4 times as much as conventional stents, and considering the volume of PCI procedures, the decision to use sirolimus-eluting stents has large economic implications.
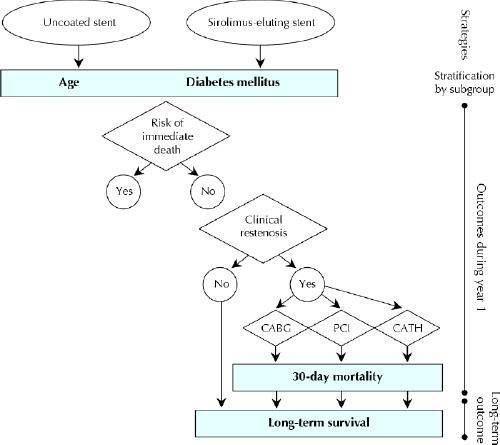
Methods: We performed an economic evaluation comparing treatment with sirolimus-eluting and conventional stents in patients undergoing PCI and in subgroups based on age and diabetes mellitus status. The probabilities of transition between clinical states and estimates of resource use and health-related quality of life were derived from the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) database. Information on effectiveness was based on a meta-analysis of randomized controlled clinical trials (RCTs) comparing sirolimus-eluting and conventional stents.
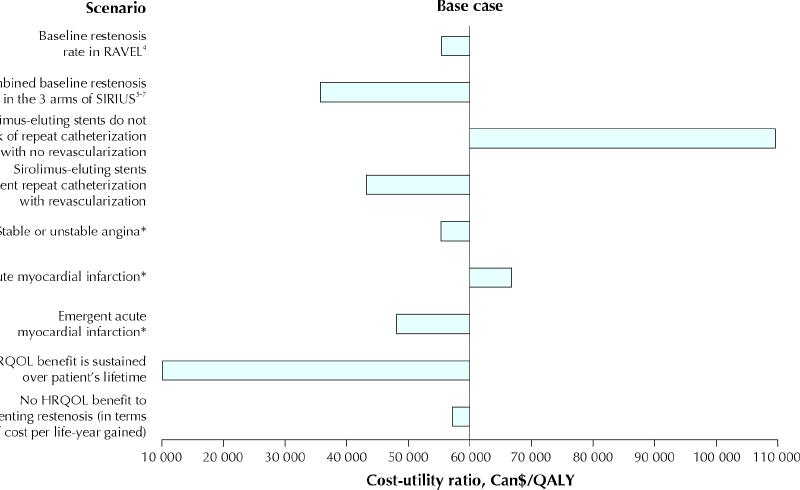
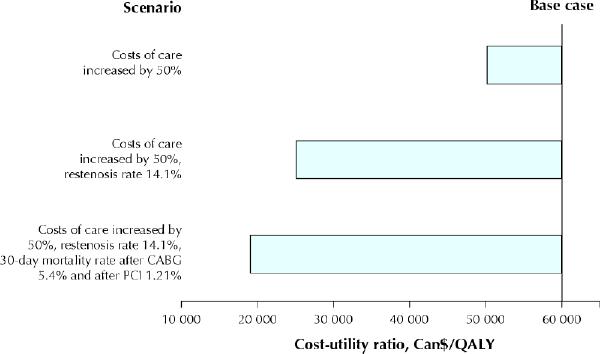
Results: Cost per quality-adjusted life year (QALY) gained in the baseline analysis was Can58,721 dollars. Sirolimus-eluting stents were more cost-effective in patients with diabetes and in those over 75 years of age, the costs per QALY gained being 44,135 dollars and 40,129 dollars, respectively. The results were sensitive to plausible variations in the cost of stents, the estimate of the effectiveness of sirolimus-eluting stents and the assumption that sirolimus-eluting stents would prevent the need for cardiac catheterizations in the subsequent year when no revascularization procedure was performed to treat restenosis.
Interpretation: The use of sirolimus-eluting stents is associated with a cost per QALY that is similar to or higher than that of other accepted medical forms of therapy and is associated with a significant incremental cost. Sirolimus-eluting stents are more economically attractive for patients who are at higher risk of restenosis or at a high risk of death if a second revascularization procedure were to be required.
Figures
Comment in
-
The dollars and sense of drug-eluting stents.CMAJ. 2005 Feb 1;172(3):361-2. doi: 10.1503/cmaj.1041486. CMAJ. 2005. PMID: 15684119 Free PMC article. No abstract available.
References
-
- Cutlip DE, Chauhan MS, Baim DS, Ho KKL, Popma JJ, Carrozza JP, et al. Clinical restenosis after coronary stenting: perspectives from multicenter clinical trials. J Am Coll Cardiol 2002;40:2082-9. - PubMed
-
- Weaver WD, Reisman MA, Griffin JJ, Buller CE, Leimgruber PP, Henry T. Optimum percutaneous transluminal coronary angioplasty compared with routine stent strategy trial (OPUS-1): a randomised trial. Lancet 2000; 355: 2199-203. - PubMed
-
- Jamal SM, Shrive FM, Ghali WA, Knudtson ML, Eisenberg MJ, for the Canadian Cardiovascular Outcomes Research Team (CCORT). In-hospital outcomes after percutaneous coronary intervention in Canada: 1992/93 to 2000/01. Can J Cardiol 2003;19:782-9. - PubMed
-
- Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-80. - PubMed
-
- Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O'Shaughnessy C, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315-23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous