

Review
doi: 10.1503/cmaj.1040752.
Liver enzyme alteration: a guide for clinicians
Affiliations
- PMID: 15684121
- PMCID: PMC545762
- DOI: 10.1503/cmaj.1040752
Item in Clipboard
Review
Liver enzyme alteration: a guide for clinicians
CMAJ.
.
Abstract
Isolated alterations of biochemical markers of liver damage in a seemingly healthy patient can present a challenge for the clinician. In this review we provide a guide to interpreting alterations to liver enzyme levels. The functional anatomy of the liver and pathophysiology of liver enzyme alteration are briefly reviewed. Using a schematic approach that classifies enzyme alterations as predominantly hepatocellular or predominantly cholestatic, we review abnormal enzymatic activity within the 2 subgroups, the most common causes of enzyme alteration and suggested initial investigations.
Figures
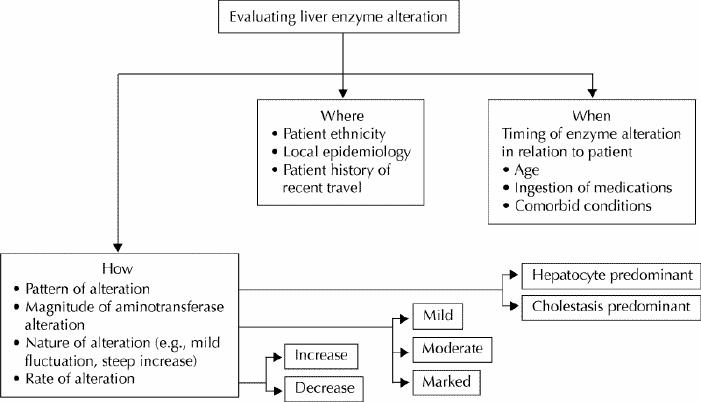
Fig. 1: Schematic representation of an approach to liver enzyme alteration. Specific modalities of enzyme alteration (how) and their relation with peculiar characteristics of the patient and locality (where and when) should be thoroughly assessed before the definitive diagnostic work-up is begun.
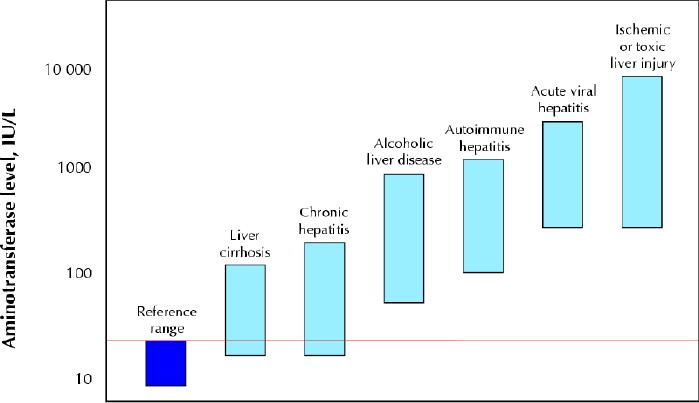
Fig. 2: Serum aminotransferase levels in various liver diseases. Patients with acute viral or ischemic or toxic liver injury reach the highest aminotransferase levels, but there is a broad overlap in aminotransferase values between patients with acute alcoholic hepatitis and autoimmune hepatitis as well as between patients with chronic hepatitis and liver cirrhosis. Both chronic hepatitis and cirrhotic patients may have aminotransferase levels within the reference range. The red line indicates the upper limit of the reference range.
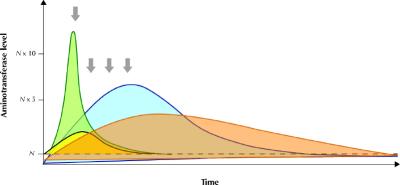
Fig. 3: Schematic representation of the rate of change of aminotransferase and bilirubin levels in a patient with acute ischemic hepatitis (green area, yellow area respectively) and acute viral hepatitis (blue area, orange area respectively). It is important to underscore that the pattern of enzyme alteration may vary and occasionally appear similar if a single observation point is taken into consideration (arrows).
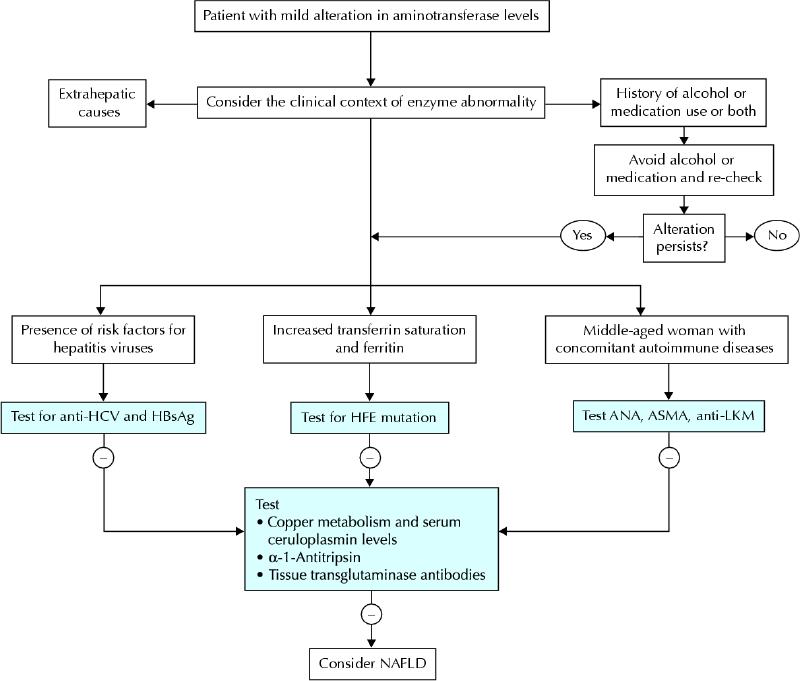
Fig. 4: Schematic, initial diagnostic algorithm for a patient presenting with mild aminotransferase abnormality. HCV = hepatitis C virus, HBsAG = hepatitis B surface antigen, ANA = antinuclear antibodies, ASMA = anti-smooth body antibodies, LKM = liver–kidney microsomes. Alcohol abuse and, to a lesser extent, drug-induced liver injury are frequently associated with mild aminotransferase abnormality, and their causality should be ruled out on a clinical basis. In the western world, chronic viral hepatitis, autoimmune hepatitis and hereditary hemochromatosis are the most common causes of mild aminotransferase alteration for which specific serological tests are available. Although nonalcoholic fatty liver disease (NAFLD) or steatohepatitis is frequently encountered in clinical practice, it remains a diagnosis of exclusion.
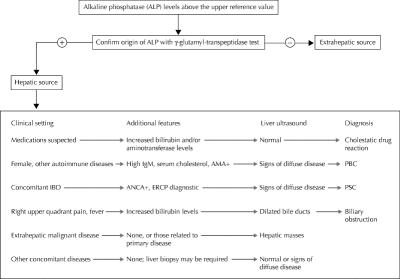
Fig. 5: Suggested diagnostic algorithm for patients presenting with increased alkaline phosphatase levels. AMA = antimitochondria antibodies, PBC = primary biliary cirrhosis, ANCA = antineutrophil cytoplasmic antibodies, ERCP = endoscopic retrograde cholangiopancreatography, PSC = primary sclerosing cholangitis.
References
-
- Green RM, Flamm S. AGA technical review on the evaluation of liver chemistry tests. Gastroenterology 2002;123(4):1367-84. - PubMed
-
- Burkitt HG, Young B, Heath JW. Wheater's functional histology: a text and colour atlas. 3rd ed. Edinburgh: Churchill Livingston, 1993.
-
- Worobetz L, Hilsden R, Shaffer E, Simon J Pare P, Scully L, et al. The liver. In Thomson BR, Shaffer EA, editors. First Principles of Gastroenterology. 2nd ed. University of Toronto Press: Toronto; 1994.
-
- Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin Chem 2000;46(12):2027-49. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical