

Quality of care provided to febrile children presenting in rural private clinics on the Kenyan coast
- PMID: 15687068
- PMCID: PMC2688335
Quality of care provided to febrile children presenting in rural private clinics on the Kenyan coast
Abstract
Background: Private sector health facilities are diverse in nature, and offer widely varying quality of care (QOC).
Objectives: The study aimed to describe the QOC provided to febrile children at rural private clinics on the Kenyan coast and stakeholder perspectives on standards of practice and opportunities for change.
Methods: Data collection methods were structured observations of consultations; interviews with users on exit from clinic and at home and in depth interviews with private practitioners (PP) and district health managers.
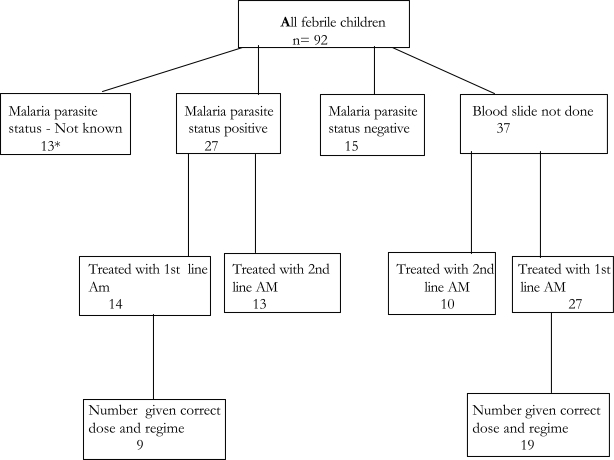
Findings: Private clinics have basic structural features for health care delivery. The majority of the clinics in this study were owned and run by single-handed trained medical practitioners. Amongst 92 observed consultations, 62% of diagnoses made were consistent with the history, examinations and tests performed. 74% of childhood fevers were diagnosed as malaria, and 88% of all prescriptions contained an antimalarial drug. Blood slides for malaria parasites were performed in 55 children (60%). Of those whose blood slide was positive (n=27), 52% and 48% were treated with a nationally recommended first or second line antimalarial drug, respectively. Where no blood slide was done (n=37), 73% were prescribed a nationally recommended first line and 27% received a second line antimalarial drug. Overall, 68 % of antimalarial drugs were prescribed in an appropriate dose and regime. Both private practitioners and district health managers expressed the view that existing linkages between the public and private health sectors within the district are haphazard and inadequate.
Conclusions: Although rural PPs are potentially well placed for treatment of febrile cases in remote settings, they exhibit varying QOC. Practitioners, users and district managers supported the need to develop interventions to improve QOC. The study identifies the need to consider involvement of the for-profit providers in the implementation of the IMCI guidelines in Kenya.
Figures
Similar articles
-
Assessing health worker performance in malaria case management of underfives at health facilities in a rural Tanzanian district.Trop Med Int Health. 2007 Jan;12(1):52-61. doi: 10.1111/j.1365-3156.2006.01753.x. Trop Med Int Health. 2007. PMID: 17207148
-
Treatment in Kenyan rural health facilities: projected drug costs using the WHO-UNICEF integrated management of childhood illness (IMCI) guidelines.Bull World Health Organ. 1999;77(10):852-8. Bull World Health Organ. 1999. PMID: 10593034 Free PMC article.
-
Malaria control in Bungoma District, Kenya: a survey of home treatment of children with fever, bednet use and attendance at antenatal clinics.Bull World Health Organ. 2001;79(11):1014-23. Bull World Health Organ. 2001. PMID: 11731808 Free PMC article.
-
Quality of treatment for febrile illness among children at outpatient facilities in sub-Saharan Africa.Ann Trop Med Parasitol. 2006 Jun;100(4):283-96. doi: 10.1179/136485906X105633. Ann Trop Med Parasitol. 2006. PMID: 16762109 Review.
-
[Analysis of ambulatory consultation length in medical clinics].Rev Med Chil. 2013 Mar;141(3):361-6. doi: 10.4067/S0034-98872013000300012. Rev Med Chil. 2013. PMID: 23900328 Review. Spanish.
Cited by
-
Tackling HIV, malaria, tuberculosis and others together.Afr Health Sci. 2004 Dec;4(3):143. Afr Health Sci. 2004. PMID: 15687064 Free PMC article. No abstract available.
-
A retrospective evaluation of the quality of malaria case management at twelve health facilities in four districts in Zambia.Asian Pac J Trop Biomed. 2014 Jun;4(6):498-504. doi: 10.12980/APJTB.4.2014C153. Asian Pac J Trop Biomed. 2014. PMID: 25182953 Free PMC article.
-
Private sector quality of care for maternal, new-born, and child health in low-and-middle-income countries: a secondary review.Front Glob Womens Health. 2024 Apr 19;5:1369792. doi: 10.3389/fgwh.2024.1369792. eCollection 2024. Front Glob Womens Health. 2024. PMID: 38707636 Free PMC article.
References
-
- Uplaker M. Private Health care. Social Science and Medicine. 2000;51:897–904. - PubMed
-
- Bennet S, Mcpake B, Mills A. Private health providers in developing countries serving the public interest? London: Zed Books; 1997.
-
- Smith E, Brugha R, Zwi A. Working with private sector providers for better health care: An introductory Guide. Options and London School of Hygiene and Tropical Medicine; 2001.
-
- Foster S. Treatment of malaria outside the formal health services. Journal of Tropical Medicine and Hygiene. 1995;98:29–34. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous