

Sex differences in patients referred for evaluation of poor growth
- PMID: 15689911
- PMCID: PMC4147725
- DOI: 10.1016/j.jpeds.2004.09.009
Sex differences in patients referred for evaluation of poor growth
Abstract
Objectives: The objective of this study was to compare sex differences among referrals for evaluation of poor growth.
Study design: This study was based on chart reviews of all new-patient encounters at Children's Hospital of Philadelphia Diagnostic and Research Growth Center for short stature or poor growth evaluations during 2001. Outcome measures were patient growth characteristics, frequency of underlying pathology, and frequency of laboratory and radiologic investigations before referral.
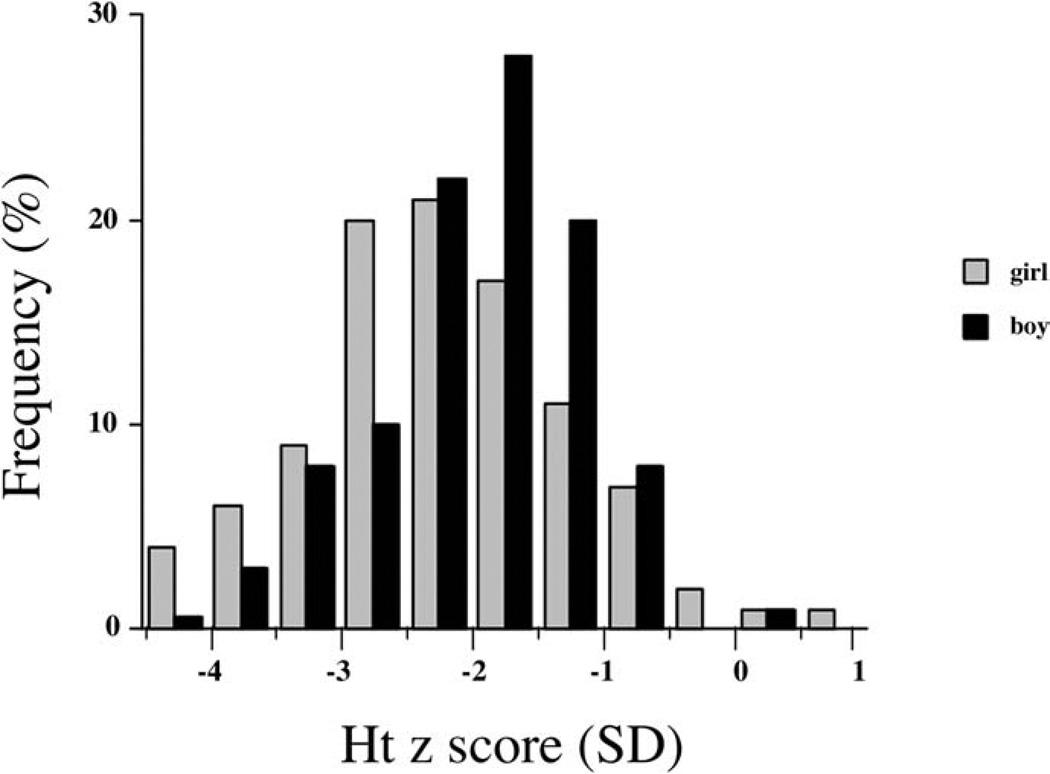
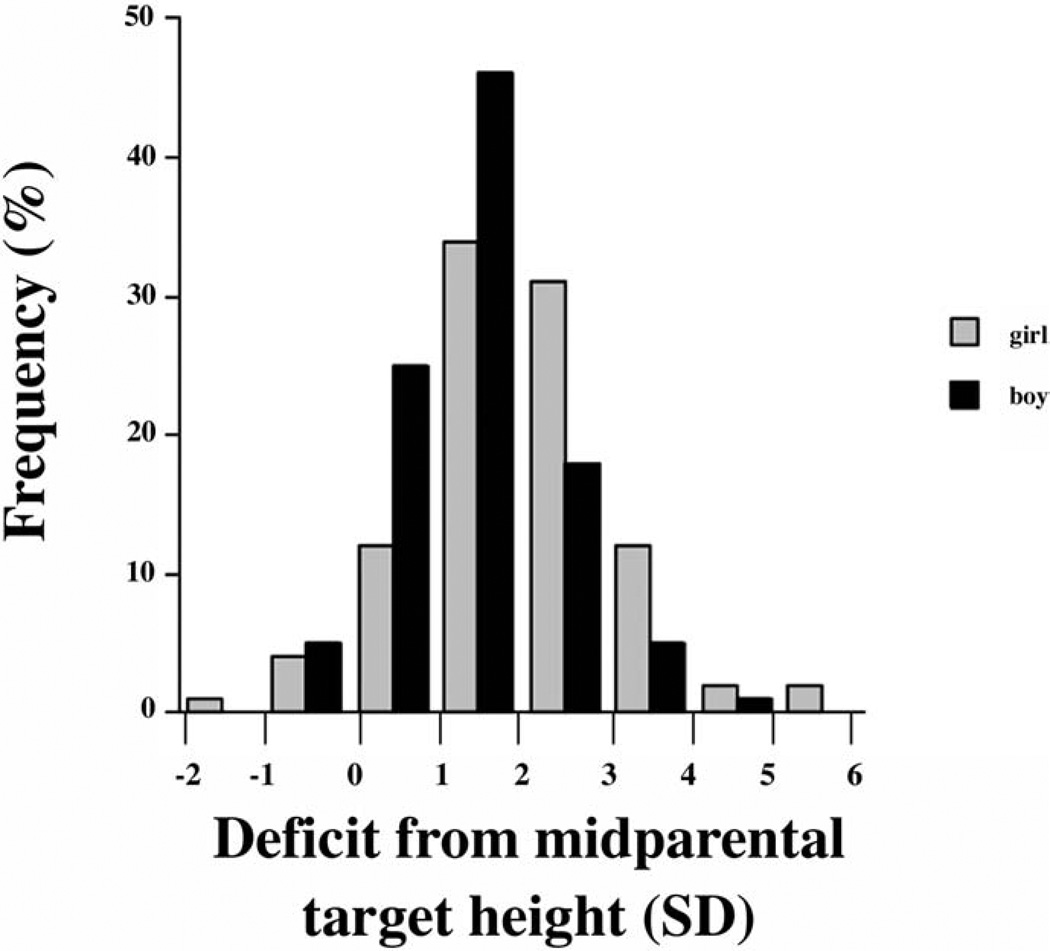
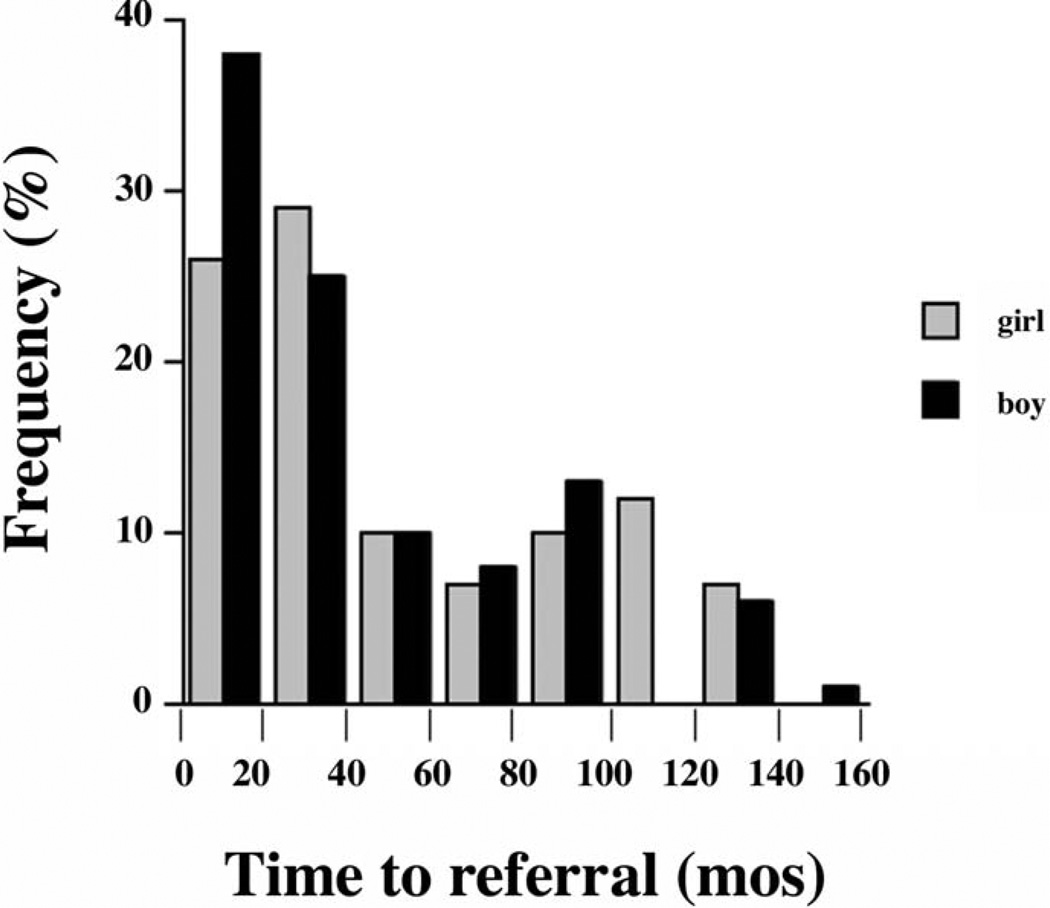
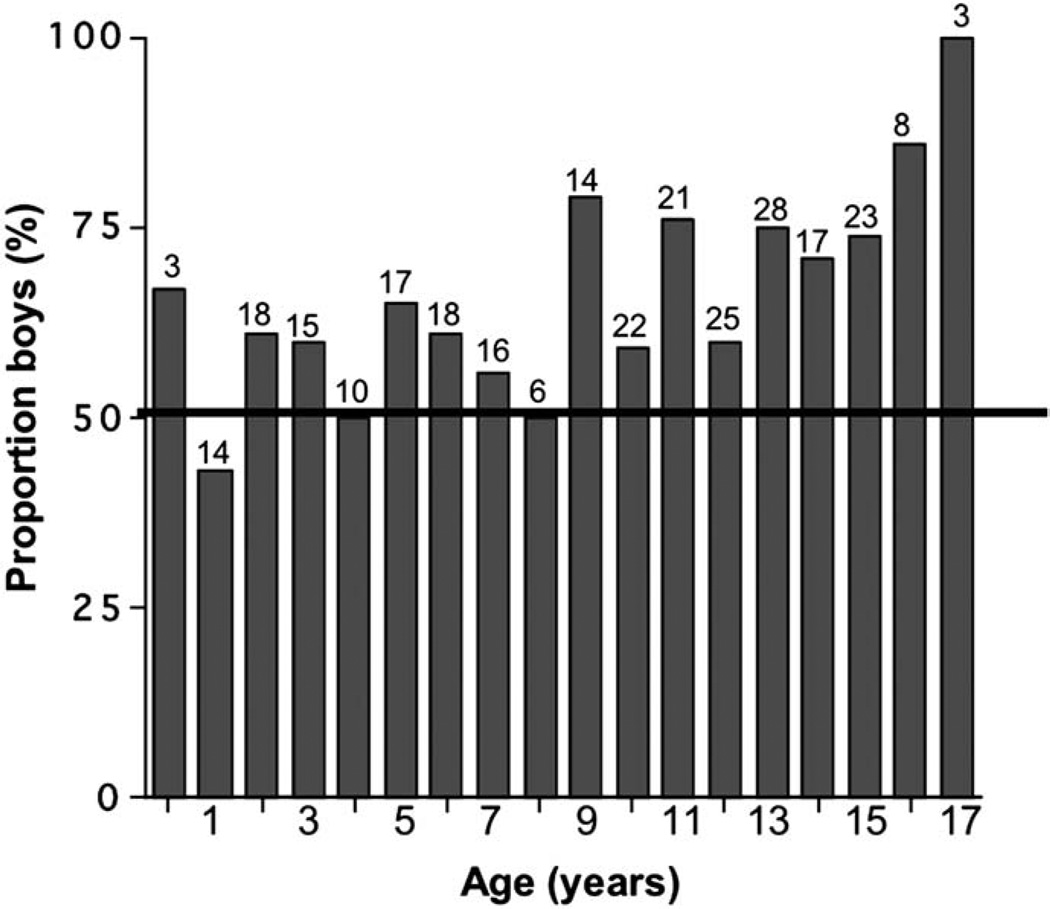
Results: One hundred eighty-two boys and 96 girls were referred ( P < .0001). Girls were shorter, relative to the general population (median height z score, -2.4 vs -1.9 for boys, P = .02) and mid-parental target heights (median deficit, 1.9 vs 1.3 SD, P < .01). Differences were more pronounced starting at age 9 years. Median time to referral from initial fall-off on the growth curve was 35 months in girls and 24 months in boys (not significant). The percentage of girls (41%) with organic disease significantly exceeded that of boys (15%). Conversely, more boys (72%) than girls (48%) were of normal height or short but healthy ( P < .0001). Sex was not associated with frequency of tests before referral; neither was severity of short stature.
Conclusions: Sex differences in short stature referrals may delay diagnosis of diseases in girls while promoting overzealous evaluations of healthy boys who do not appear to be tall enough.
Figures
Similar articles
-
Referrals for tall stature in children: a 25-year personal experience.J Paediatr Child Health. 2009 Jan-Feb;45(1-2):58-63. doi: 10.1111/j.1440-1754.2008.01428.x. J Paediatr Child Health. 2009. PMID: 19208068
-
Threshold of evaluation for short stature in a pediatric endocrine clinic: differences between boys versus girls?J Pediatr Endocrinol Metab. 2007 Jan;20(1):21-6. doi: 10.1515/jpem.2007.20.1.21. J Pediatr Endocrinol Metab. 2007. PMID: 17315525
-
Accuracy of final height prediction and effect of growth-reductive therapy in 362 constitutionally tall children.J Clin Endocrinol Metab. 1996 Mar;81(3):1206-16. doi: 10.1210/jcem.81.3.8772601. J Clin Endocrinol Metab. 1996. PMID: 8772601
-
[Frequent growth disorders in puberty and adolescence].Padiatr Padol. 1991;26(3):125-30. Padiatr Padol. 1991. PMID: 1945473 Review. German.
-
Etiologies and early diagnosis of short stature and growth failure in children and adolescents.J Pediatr. 2014 May;164(5 Suppl):S1-14.e6. doi: 10.1016/j.jpeds.2014.02.027. J Pediatr. 2014. PMID: 24731744 Review.
Cited by
-
Gender Bias in U.S. Pediatric Growth Hormone Treatment.Sci Rep. 2015 Jun 9;5:11099. doi: 10.1038/srep11099. Sci Rep. 2015. PMID: 26057697 Free PMC article.
-
Safety and Efficacy of Lonapegsomatropin in Children With Growth Hormone Deficiency: enliGHten Trial 2-Year Results.J Clin Endocrinol Metab. 2022 Jun 16;107(7):e2680-e2689. doi: 10.1210/clinem/dgac217. J Clin Endocrinol Metab. 2022. PMID: 35428884 Free PMC article. Clinical Trial.
-
Medically underserved girls receive less evaluation for short stature.Pediatrics. 2011 Apr;127(4):696-702. doi: 10.1542/peds.2010-1563. Epub 2011 Mar 21. Pediatrics. 2011. PMID: 21422085 Free PMC article.
-
Variation in methods of predicting adult height for children with idiopathic short stature.Pediatrics. 2010 Nov;126(5):938-44. doi: 10.1542/peds.2009-3649. Epub 2010 Oct 25. Pediatrics. 2010. PMID: 20974789 Free PMC article.
-
Evaluation of referrals for short stature: A retrospective chart review.Paediatr Child Health. 2019 May;24(2):e74-e77. doi: 10.1093/pch/pxy079. Epub 2018 Jun 13. Paediatr Child Health. 2019. PMID: 30996610 Free PMC article.
References
-
- Kanof ME, Lake AM, Bayless TM. Decreased height velocity in children and adolescents before the diagnosis of Crohn’s disease. Gastroenterology. 1988;95:1523–1527. - PubMed
-
- Bonamico M, Scire G, Mariani P, Pasquino AM, Triglione P, Scaccia S, et al. Short stature as the primary manifestation of monosymptomatic celiac disease. J Pediatr Gastroenterol Nutr. 1992;14:12–16. - PubMed
-
- Giglio L, Candusso M, D’Orazio C, Mastella G, Faraguna D. Failure to thrive: the earliest feature of cystic fibrosis in infants diagnosed by neonatal screening. Acta Paediatr. 1997;86:1162–1165. - PubMed
-
- Roth KS, Chan JC. Renal tubular acidosis: a new look at an old problem. Clin Pediatr. 2001;40:533–543. - PubMed
-
- Arpadi SM. Growth failure in children with HIV infection. JAIDS. 2000;25(Suppl 1):S37–S42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
