

A novel surgical procedure for bridging of massive bone defects
- PMID: 15691380
- PMCID: PMC550665
- DOI: 10.1186/1477-7819-3-7
A novel surgical procedure for bridging of massive bone defects
Abstract
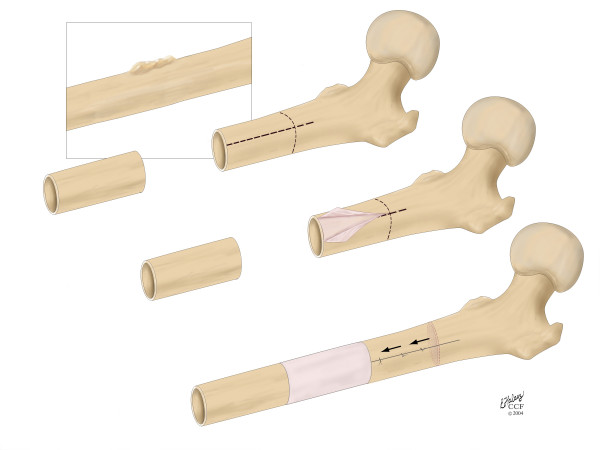
BACKGROUND: Bony defects arising from tumor resection or debridement after infection, non-union or trauma present a challenging problem to orthopedic surgeons, as well as patients due to compliance issues. Current treatment options are time intensive, require more than one operation and are associated with high rate of complications. For this reason, we developed a new surgical procedure to bridge a massive long bone defect. METHODS: To bridge the gap, an in situ periosteal sleeve is elevated circumferentially off of healthy diaphyseal bone adjacent to the bone defect. Then, the adjacent bone is osteotomized and the transport segment is moved along an intramedullary nail, out of the periosteal sleeve and into the original diaphyseal defect, where it is docked. Vascularity is maintained through retention of the soft tissue attachments to the in situ periosteal sleeve. In addition, periosteal osteogenesis can be augmented through utilization of cancellous bone graft or in situ cortical bone adherent to the periosteal sleeve. RESULTS: The proposed procedure is novel in that it exploits the osteogenic potential of the periosteum by replacing the defect arising from resection of tissue out of a pathological area with a defect in a healthy area of tissue, through transport of the adjacent bone segment. Furthermore, the proposed procedure has several advantages over the current standard of care including ease of implementation, rapid patient mobilization, and no need for specialized implants (intramedullary nails are standard inventory for surgical oncology and trauma departments) or costly orthobiologics. CONCLUSIONS: The proposed procedure offers a viable and potentially preferable alternative to the current standard treatment modalities, particularly in areas of the world where few surgeons are trained for procedures such as distraction osteogenesis (e.g. the Ilizarov procedure) as well as areas of the world where surgeons have little access to expensive, complex devices and orthobiologics.
Figures
References
-
- Salkeld SL, Patron LP, Cook SD. The effect of osteogenic protein-1 on the healing of segmental bone defects treated with allograft bone. J Bone Joint Surg Am. 2001;83-A:803–816. - PubMed
-
- Klaue K, Knothe U, Anton C, Masquelet AC, Petten SM. Biological implementation of autologous foreign body membranes in corticalization of massive cancellous bone grafts. Trans Orthopedic Trauma Association. 1996.
-
- Hertel R, Knothe U, Gerber A, Cordey J, Rahn R. The osteogenic potential of vascularized periosteum and cancellous bone graft in sheep. Trans Orthopedic Research Society. 1997.
LinkOut - more resources
Full Text Sources
Miscellaneous
