

Factors affecting posttransfusion platelet increments, platelet refractoriness, and platelet transfusion intervals in thrombocytopenic patients
- PMID: 15692069
- PMCID: PMC1895076
- DOI: 10.1182/blood-2003-08-2724
Factors affecting posttransfusion platelet increments, platelet refractoriness, and platelet transfusion intervals in thrombocytopenic patients
Abstract
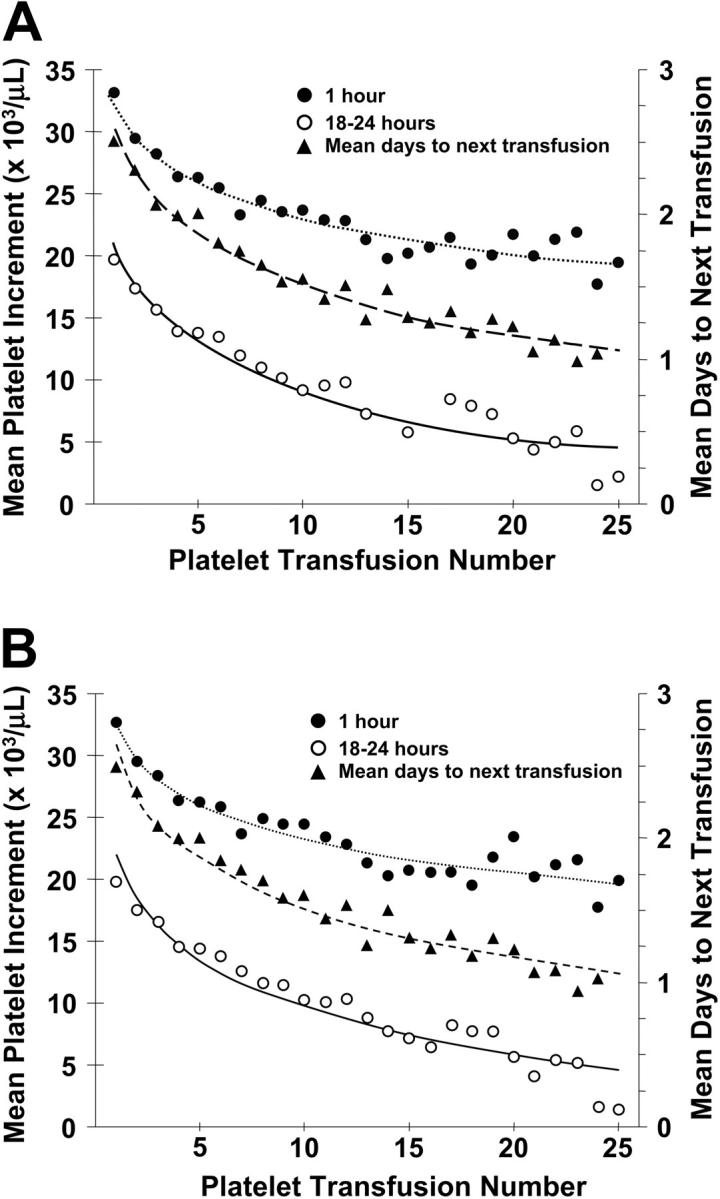
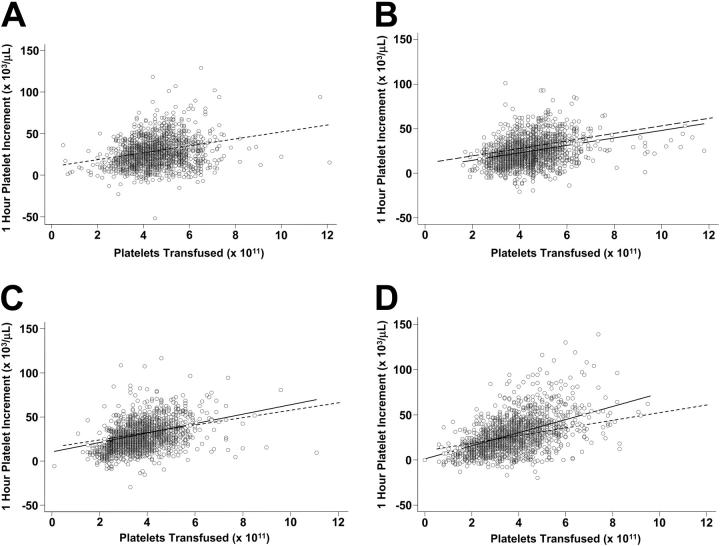
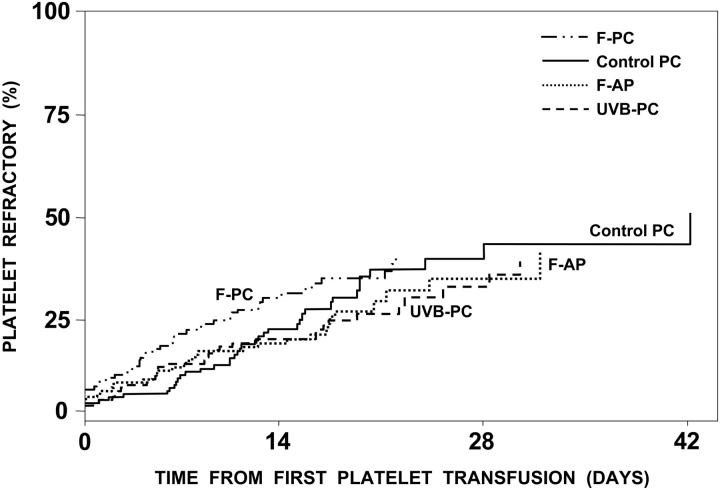
A variety of patient and product-related factors influenced the outcome of 6379 transfusions given to 533 patients in the Trial to Reduce Alloimmunization to Platelets (TRAP). Responses measured were platelet increments, interval between platelet transfusions, and platelet refractoriness. Patient factors that improved platelet responses were splenectomy and increasing patient age. In contrast, at least 2 prior pregnancies, male gender, splenomegaly, bleeding, fever, infection, disseminated intravascular coagulation, increasing height and weight, lymphocytotoxic antibody positivity, an increasing number of platelet transfusions, or receiving heparin or amphotericin were associated with decreased posttransfusion platelet responses. Platelet factors that were associated with improved platelet responses were giving ABO-compatible platelets, platelets stored for 48 hours or less, and giving large doses of platelets while ultraviolet B (UV-B) or gamma irradiation decreased platelet responses. However, in alloimmunized lymphocytoxic antibody-positive patients, the immediate increment to UV-B-irradiated platelets was well maintained, whereas all other products showed substantial reductions. Refractoriness to platelet transfusions developed in 27% of the patients. Platelet refractoriness was associated with lymphocytotoxic antibody positivity, heparin administration, fever, bleeding, increasing number of platelet transfusions, increasing weight, at least 2 pregnancies, and male gender. The only factors that reduced platelet refractoriness rates were increasing the dose of platelets transfused or transfusing filtered apheresis platelets.
Figures
Comment in
-
Leucoreduction of blood components: an effective way to increase blood safety?Blood Transfus. 2016 May;14(2):214-27. doi: 10.2450/2015.0154-15. Epub 2015 Dec 16. Blood Transfus. 2016. PMID: 26710353 Free PMC article. Review.
References
-
- The Trial to Reduce Alloimmunization to Platelets Study Group. Leukocyte reduction and ultraviolet B irradiation of platelets to prevent alloimmunization and refractoriness to platelet transfusions. N Engl J Med. 1997;337: 1861-1869. - PubMed
-
- Murphy S, Heaton WA, Rebulla P. Platelet production in the old world—and the new. Transfusion. 1996;36: 751-754. - PubMed
-
- Davis KB, Slichter SJ, Corash L. Corrected count increment and percent platelet recovery as measures of post-transfusion platelet response: problems and a solution. Transfusion. 1999;39: 586-592. - PubMed
-
- Yankee RA, Grumet FC, Rogentine GN. Platelet transfusion therapy: the selection of compatible donors for refractory patients by lymphocyte HLA typing. N Engl J Med. 1969;281: 1208-1212. - PubMed
-
- Slichter SJ. Platelet production, physiology, hemostasis, and transfusion therapy. In: Spiess BD, Counts RB, Gould SA, eds. Perioperative Transfusion Medicine. Baltimore, MD: Williams & Wilkins; 1998: 61-77.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
