

Targeting the silent minority: emerging immunotherapeutic strategies for eradication of malignant stem cells in chronic myeloid leukaemia
- PMID: 15692843
- PMCID: PMC11032986
- DOI: 10.1007/s00262-004-0573-1
Targeting the silent minority: emerging immunotherapeutic strategies for eradication of malignant stem cells in chronic myeloid leukaemia
Abstract
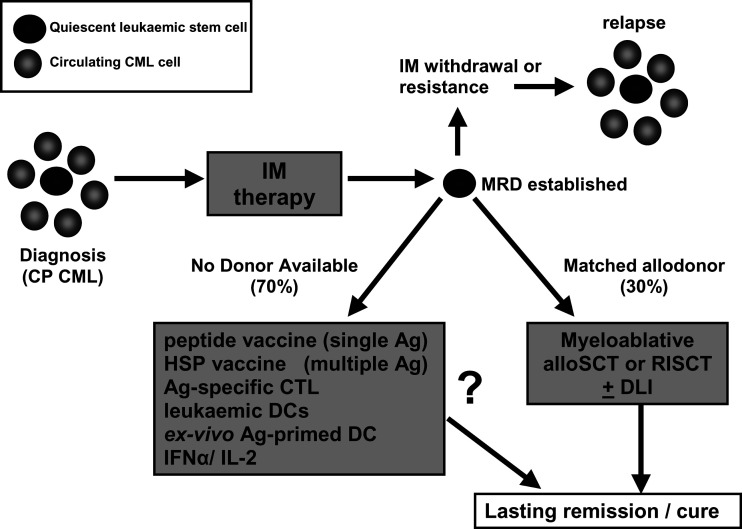
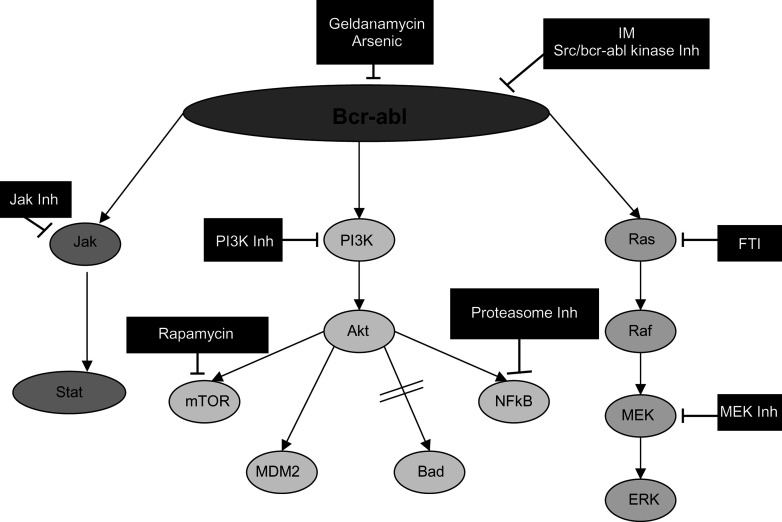
Standard allogeneic stem cell transplantation (alloSCT) has provided a cure for chronic myeloid leukaemia (CML) over the last 25 years, but is only an option for a minority of patients. It was hoped that the introduction of imatinib mesylate (IM), a specific tyrosine kinase inhibitor that targets the Bcr-Abl oncogene product, would provide long-term remission or even cure for those patients without a donor, but studies have shown that IM does not eliminate leukaemic stem cells in CML patients. To overcome this problem of molecular persistence, research is underway to combine reduced intensity stem cell transplant or non-donor-dependent immunotherapies with IM with the aim of increasing cure rate, reducing toxicity and improving quality of life. The alternative approach is to combine IM or second-generation agents with other novel drugs that interrupt key signalling pathways activated by Bcr-Abl. This article will focus on the latest immunotherapy and molecularly targeted therapeutic options in CML and how they may be combined to improve the outcome for CML patients in the future.
Figures
Similar articles
-
Targeted chronic myeloid leukemia therapy: seeking a cure.J Manag Care Pharm. 2007 Oct;13(8 Suppl A):8-12. doi: 10.18553/jmcp.2007.13.s8-a.8. J Manag Care Pharm. 2007. PMID: 17970609 Free PMC article. Review.
-
Persistence of malignant hematopoietic progenitors in chronic myelogenous leukemia patients in complete cytogenetic remission following imatinib mesylate treatment.Blood. 2003 Jun 15;101(12):4701-7. doi: 10.1182/blood-2002-09-2780. Epub 2003 Feb 6. Blood. 2003. PMID: 12576334
-
BCR-ABL kinase domain mutations, including 2 novel mutations in imatinib resistant Malaysian chronic myeloid leukemia patients-Frequency and clinical outcome.Leuk Res. 2014 Apr;38(4):454-9. doi: 10.1016/j.leukres.2013.12.025. Epub 2014 Jan 6. Leuk Res. 2014. PMID: 24456693
-
Characterization of cancer stem cells in chronic myeloid leukaemia.Biochem Soc Trans. 2007 Nov;35(Pt 5):1347-51. doi: 10.1042/BST0351347. Biochem Soc Trans. 2007. PMID: 17956348 Review.
-
Chronic myelogenous leukemia.Curr Opin Oncol. 2001 Jan;13(1):3-7. doi: 10.1097/00001622-200101000-00002. Curr Opin Oncol. 2001. PMID: 11148678 Review.
Cited by
-
Bedside to bench: interfering with leukemic stem cells.Nat Med. 2008 May;14(5):494-5. doi: 10.1038/nm0508-494. Nat Med. 2008. PMID: 18463658 Free PMC article.
-
CD34(+)/CD38(-) stem cells in chronic myeloid leukemia express Siglec-3 (CD33) and are responsive to the CD33-targeting drug gemtuzumab/ozogamicin.Haematologica. 2012 Feb;97(2):219-26. doi: 10.3324/haematol.2010.035006. Epub 2011 Oct 11. Haematologica. 2012. PMID: 21993666 Free PMC article.
-
A novel co-operative mechanism linking TGFβ and Lyn kinase activation to imatinib resistance in chronic myeloid leukaemia cells.Oncotarget. 2012 May;3(5):518-24. doi: 10.18632/oncotarget.500. Oncotarget. 2012. PMID: 22643838 Free PMC article.
-
Administration of embryonic stem cells generates effective antitumor immunity in mice with minor and heavy tumor load.Cancer Immunol Immunother. 2010 Nov;59(11):1697-705. doi: 10.1007/s00262-010-0899-9. Epub 2010 Aug 4. Cancer Immunol Immunother. 2010. PMID: 20683592 Free PMC article.
References
-
- Appel S, Boehmler AM, Grunebach F, Muller MR, Rupf A, Weck MM, Hartmann U, Reichardt VL, Kanz L, Brummendorf TH, Brossart P. Imatinib mesylate affects the development and function of dendritic cells generated from CD34+ peripheral blood progenitor cells. Blood. 2004;103:538–544. - PubMed
-
- Avery S, Nadal E, Davis J, Apperley J, Goldman J, Marin D. Infusion of peripheral blood stem cells collected at diagnosis can improve the level of cytogenetic response in CML patients on imatinib whose treatment is limited by cytopaenia. Blood. 2003;102:318b.
-
- Bakalova R, Ohba H, Zhelev Z, Ishikawa M, Shinohara Y, Baba Y. Cross-talk between Bcr-Abl tyrosine kinase, protein kinase C and telomerase-a potential reason for resistance to Glivec in chronic myelogenous leukaemia. Biochem Pharmacol. 2003;66:1879–1884. - PubMed
-
- Barrett AJ, van Rhee F. Graft-versus-leukaemia. Baillieres Clin Haematol. 1997;10:337–355. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
