

Pro-atrial natriuretic peptide is a prognostic marker in sepsis, similar to the APACHE II score: an observational study
- PMID: 15693965
- PMCID: PMC1065109
- DOI: 10.1186/cc3015
Pro-atrial natriuretic peptide is a prognostic marker in sepsis, similar to the APACHE II score: an observational study
Erratum in
- Crit Care. 2005 Apr;9(2):169
Abstract
Introduction: Additional biomarkers in sepsis are needed to tackle the challenges of determining prognosis and optimizing selection of high-risk patients for application of therapy. In the present study, conducted in a cohort of medical intensive care unit patients, our aim was to compare the prognostic value of mid-regional pro-atrial natriuretic peptide (ANP) levels with those of other biomarkers and physiological scores.
Methods: Blood samples obtained in a prospective observational study conducted in 101 consecutive critically ill patients admitted to the intensive care unit were analyzed. The prognostic value of pro-ANP levels was compared with that of the Acute Physiology and Chronic Health Evaluation (APACHE) II score and with those of various biomarkers (i.e. C-reactive protein, IL-6 and procalcitonin). Mid-regional pro-ANP was detected in EDTA plasma from all patients using a new sandwich immunoassay.
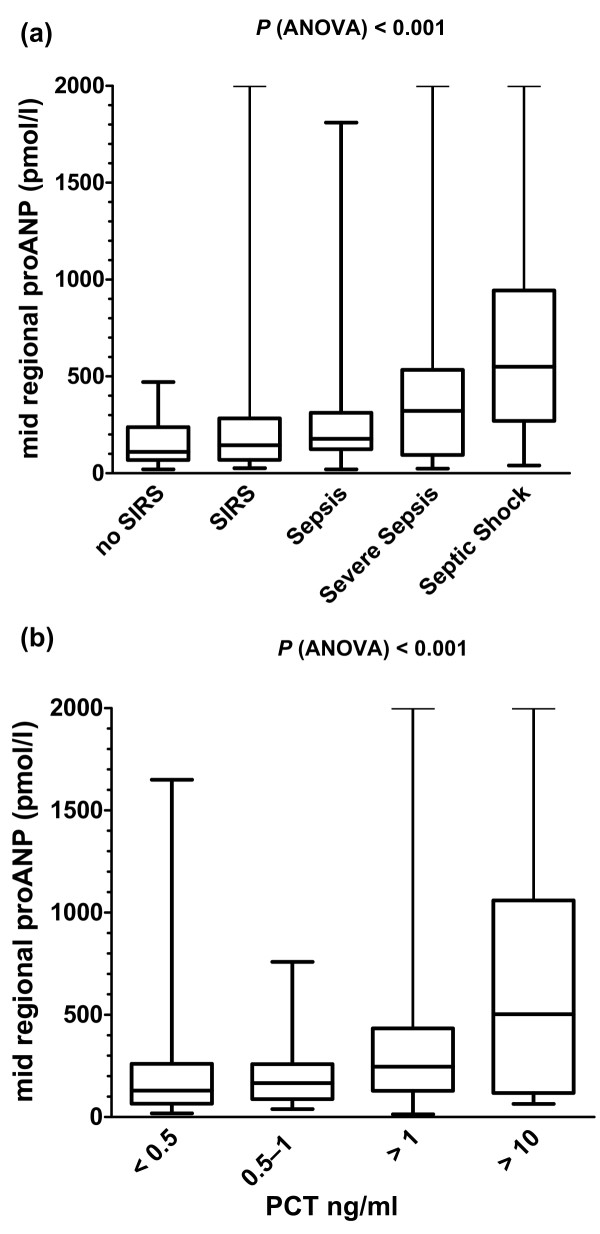
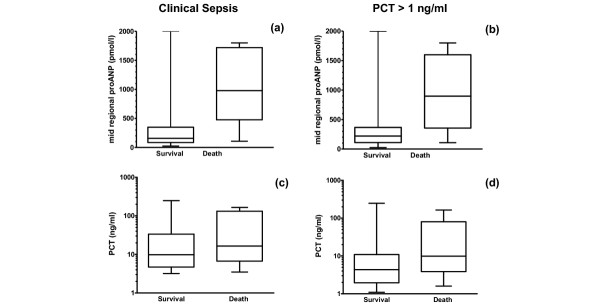
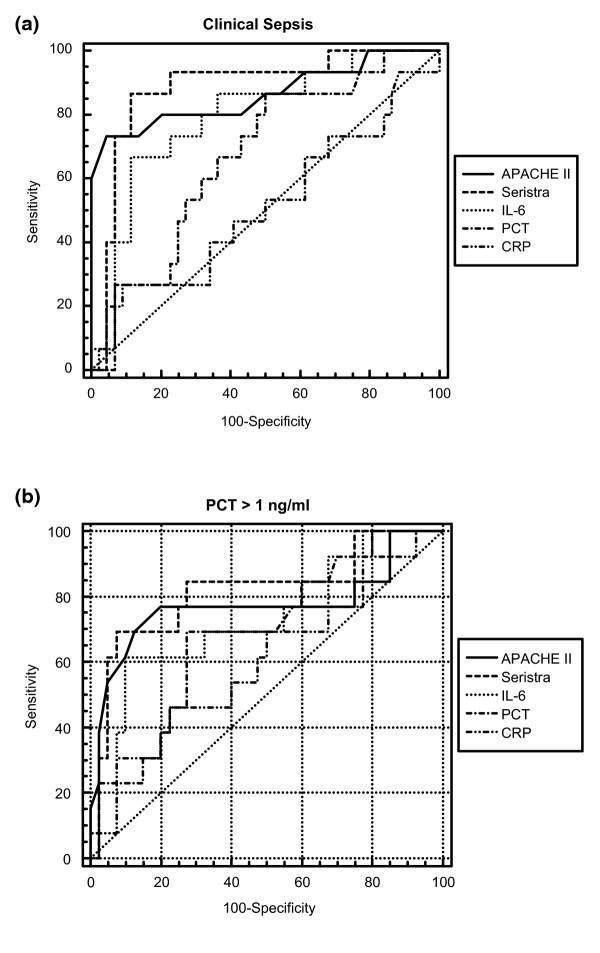
Results: On admission, 53 patients had sepsis, severe sepsis, or septic shock, and 68 had systemic inflammatory response syndrome. The median pro-ANP value in the survivors was 194 pmol/l (range 20-2000 pmol/l), which was significantly lower than in the nonsurvivors (median 853.0 pmol/l, range 100-2000 pmol/l; P < 0.001). On the day of admission, pro-ANP levels, but not levels of other biomarkers, were significantly higher in non-surviving [corrected] than in surviving [corrected] sepsis patients (P = 0.001). In a receiver operating characteristic curve analysis for the survival of patients with sepsis, the area under the curve (AUC) for pro-ANP was 0.88, which was significantly greater than the AUCs for procalcitonin and C-reactive protein, and similar to the AUC for the APACHE II score.
Conclusion: Pro-ANP appears to be a valuable tool for individual risk assessment in sepsis patients and for stratification of high-risk patients in future intervention trials. Further studies are needed to validate our results.
Figures
Similar articles
-
Mid-regional pro-adrenomedullin as a prognostic marker in sepsis: an observational study.Crit Care. 2005;9(6):R816-24. doi: 10.1186/cc3885. Epub 2005 Nov 15. Crit Care. 2005. PMID: 16356231 Free PMC article.
-
Prediction about severity and outcome of sepsis by pro-atrial natriuretic peptide and pro-adrenomedullin.Chin J Traumatol. 2010 Jun 1;13(3):152-7. Chin J Traumatol. 2010. PMID: 20515592
-
Prognostic importance of increased plasma amino-terminal pro-brain natriuretic peptide levels in a large noncardiac, general intensive care unit population.Shock. 2009 Apr;31(4):342-7. doi: 10.1097/SHK.0b013e31818635b6. Shock. 2009. PMID: 18791494
-
[Usefulness of biomarkers of sepsis in the ICU].Rev Med Suisse. 2011 Dec 14;7(321):2430-4. Rev Med Suisse. 2011. PMID: 22279860 Review. French.
-
Natriuretic peptides in septic patients.Curr Med Chem. 2009;16(30):4020-31. doi: 10.2174/092986709789352330. Curr Med Chem. 2009. PMID: 19747125 Review.
Cited by
-
Pro-atrial natriuretic peptide and pro-adrenomedullin before cardiac surgery in children. Can we predict the future?PLoS One. 2020 Jul 23;15(7):e0236377. doi: 10.1371/journal.pone.0236377. eCollection 2020. PLoS One. 2020. PMID: 32702064 Free PMC article.
-
Prohormones for prediction of adverse medical outcome in community-acquired pneumonia and lower respiratory tract infections.Crit Care. 2010;14(3):R106. doi: 10.1186/cc9055. Epub 2010 Jun 8. Crit Care. 2010. PMID: 20529344 Free PMC article. Clinical Trial.
-
Cardiovascular Biomarkers: Lessons of the Past and Prospects for the Future.Int J Mol Sci. 2022 May 19;23(10):5680. doi: 10.3390/ijms23105680. Int J Mol Sci. 2022. PMID: 35628490 Free PMC article. Review.
-
Circulating corin concentration is associated with risk of mortality and acute kidney injury in critically ill patients.Sci Rep. 2024 Aug 27;14(1):19848. doi: 10.1038/s41598-024-70587-0. Sci Rep. 2024. PMID: 39191876 Free PMC article.
-
Natriuretic peptide testing for the evaluation of critically ill patients with shock in the intensive care unit: a prospective cohort study.Crit Care. 2006 Feb;10(1):R37. doi: 10.1186/cc4839. Crit Care. 2006. PMID: 16507171 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
