

Timing of tracheostomy as a determinant of weaning success in critically ill patients: a retrospective study
- PMID: 15693966
- PMCID: PMC1065112
- DOI: 10.1186/cc3018
Timing of tracheostomy as a determinant of weaning success in critically ill patients: a retrospective study
Abstract
Introduction: Tracheostomy is frequently performed in critically ill patients for prolonged intubation. However, the optimal timing of tracheostomy, and its impact on weaning from mechanical ventilation and outcomes in critically ill patients who require mechanical ventilation remain controversial.
Methods: The medical records of patients who underwent tracheostomy in the medical intensive care unit (ICU) of a tertiary medical centre from July 1998 to June 2001 were reviewed. Clinical characteristics, length of stay in the ICU, rates of post-tracheostomy pneumonia, weaning from mechanical ventilation and mortality rates were analyzed.
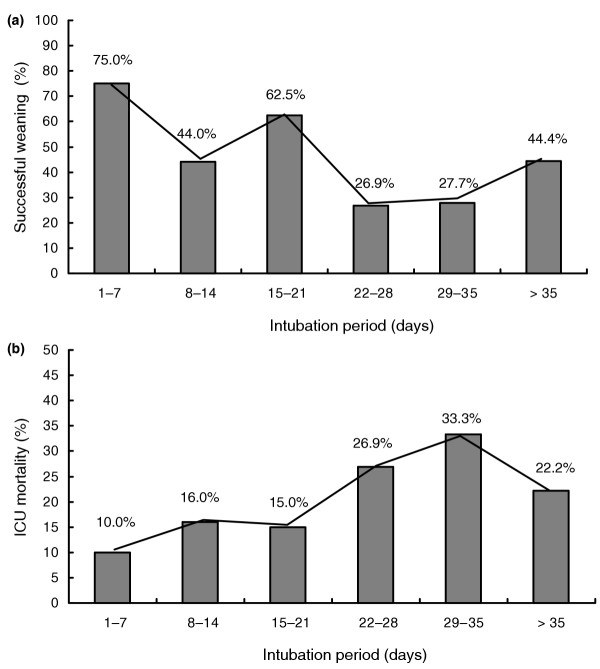
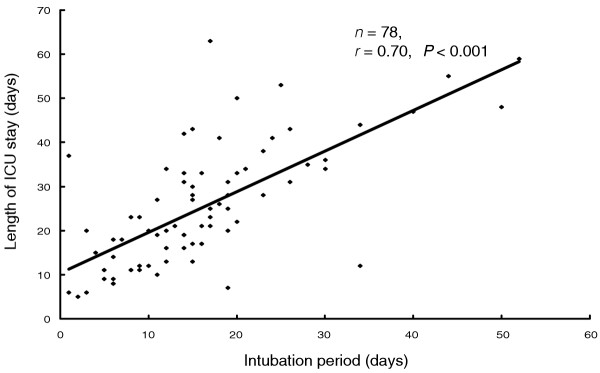
Results: A total of 163 patients (93 men and 70 women) were included; their mean age was 70 years. Patients were classified into two groups: successful weaning (n = 78) and failure to wean (n = 85). Shorter intubation periods (P = 0.02), length of ICU stay (P = 0.001) and post-tracheostomy ICU stay (P = 0.005) were noted in patients in the successful weaning group. Patients who underwent tracheostomy more than 3 weeks after intubation had higher ICU mortality rates and rates of weaning failure. The length of intubation correlated with the length of ICU stay in the successful weaning group (r = 0.70; P < 0.001). Multivariate analysis revealed that tracheostomy after 3 weeks of intubation, poor oxygenation before tracheostomy (arterial oxygen tension/fractional inspired oxygen ratio <250) and occurrence of nosocomial pneumonia after tracheostomy were independent predictors of weaning failure.
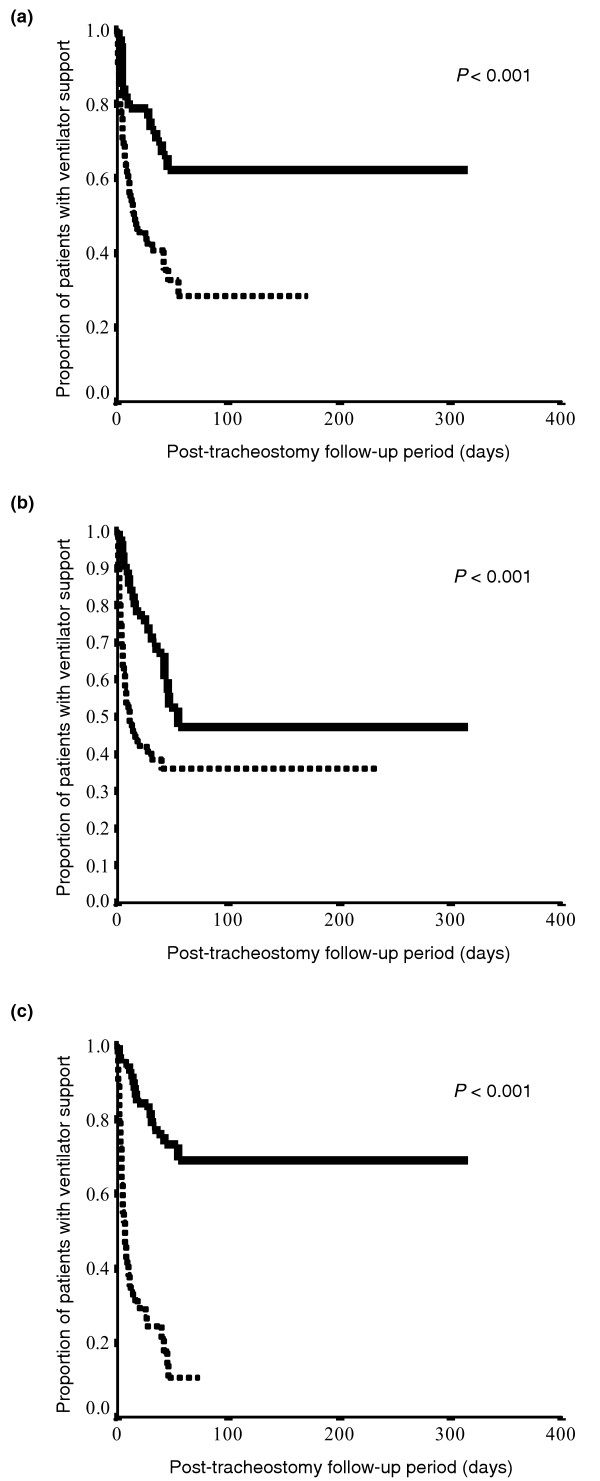
Conclusion: The study suggests that tracheostomy after 21 days of intubation is associated with a higher rate of failure to wean from mechanical ventilation, longer ICU stay and higher ICU mortality.
Figures
References
-
- Esteban A, Anzueto A, Alia I, Gordo F, Apezteguia C, Palizas F, Cide D, Goldwaser R, Soto L, Bugedo G, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161:1450–1458. - PubMed
-
- Heffner JE, Miller KS, Sahn SA. Tracheostomy in the intensive care unit. Part 1: Indications, technique, management. Chest. 1986;90:269–274. - PubMed
-
- Heffner JE. Medical indications for tracheotomy. Chest. 1989;96:186–190. - PubMed
-
- Astrachan DI, Kirchner JC, Goodwin WJ., Jr Prolonged intubation vs. tracheotomy: complications, practical and psychological considerations. Laryngoscope. 1988;98:1165–1169. - PubMed
-
- Diehl JL, El Atrous S, Touchard D, Lemaire F, Brochard L. Changes in the work of breathing induced by tracheotomy in ventilator-dependent patients. Am J Respir Crit Care Med. 1999;159:383–388. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
