

Follow up of people aged 65 and over with a history of emergency admissions: analysis of routine admission data
- PMID: 15695276
- PMCID: PMC548180
- DOI: 10.1136/bmj.330.7486.289
Follow up of people aged 65 and over with a history of emergency admissions: analysis of routine admission data
Abstract
Objective: To determine the subsequent pattern of emergency admissions in older people with a history of frequent emergency admissions.
Design: Analysis of routine admissions data from NHS hospitals using hospital episode statistics (HES) in England.
Subjects: Individual patients aged > or = 65, > or = 75, and > or = 85 who had at least two emergency admissions in 1997-8.
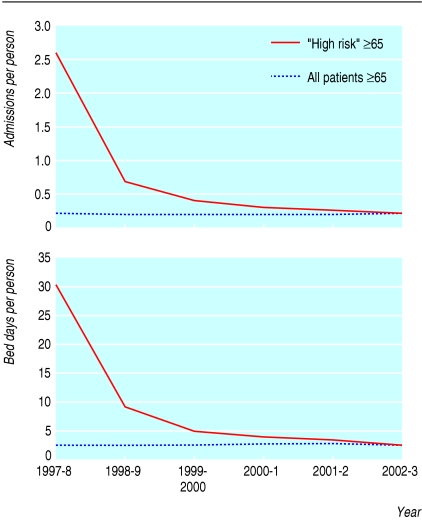
Main outcome measures: Emergency admissions and bed use in this "high risk" cohort of patients were counted for the next five years and compared with the general population of the same age. No account was taken of mortality as the analysis was designed to estimate the future use of beds in this high risk cohort.
Results: Over four to five years, admission rates and bed use in the high risk cohorts fell to the mean rate for older people. Although patients > or = 65 with two or more such admissions were responsible for 38% of admissions in the index year, they were responsible for fewer than 10% of admissions in the following year and just over 3% five years later.
Conclusion: Patients with multiple emergency admissions are often identified as a high risk group for subsequent admission and substantial claims are made for interventions designed to avoid emergency admission in such patients. Simply monitoring admission rates cannot assess interventions designed to reduce admission among frail older people as rates fall without any intervention. Comparison with a matched control group is necessary. Wider benefits than reduced admissions should be considered when introducing intensive case management of older people.
Figures
Comment in
-
Identifying people at high risk of emergency hospital admission.BMJ. 2005 Feb 5;330(7486):266. doi: 10.1136/bmj.330.7486.266. BMJ. 2005. PMID: 15695251 Free PMC article. No abstract available.
References
-
- Johri M, Beland F, Bergman H. International experiments in integrated care for the elderly: a synthesis of the evidence. Int J Geriatr Psychiatry 2003;18: 222-35. - PubMed
-
- Hutt R, Rosen R, McCauley J. Case managing long term conditions. London: King's Fund, 2004.
-
- Pacala JT, Boult C, Boult L. Predictive validity of a questionnaire that identifies older persons at risk of hospital admission. J Am Geriatr Soc 1995;43: 374-7. - PubMed
-
- Brody KK, Johnson RE, Ried LD, Carder PC, Perrin N. A comparison of two methods for identifying frail Medicare aged persons. J Am Geriatr Soc 2002;50: 562-9. - PubMed
-
- Meldon SW, Mion LC, Palmer RM, Drew BL, Connor JT, Lewiwicki LJ, et al. A brief risk stratification tool to predict repeat emergency department visits and hospitalisations in older patients discharged from the emergency room. Acad Emerg Med 2003;10: 224-32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources