

Hypercapnic acidosis impairs plasma membrane wound resealing in ventilator-injured lungs
- PMID: 15695495
- PMCID: PMC2718480
- DOI: 10.1164/rccm.200309-1223OC
Hypercapnic acidosis impairs plasma membrane wound resealing in ventilator-injured lungs
Abstract
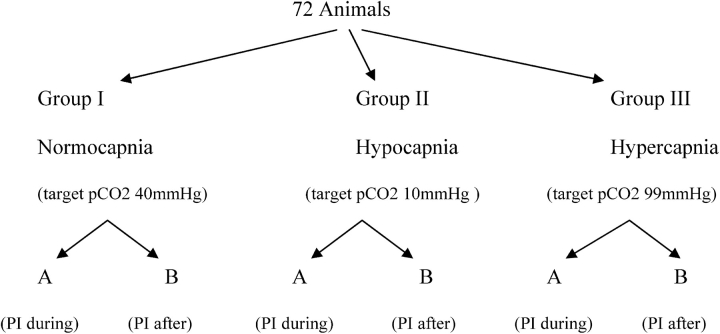
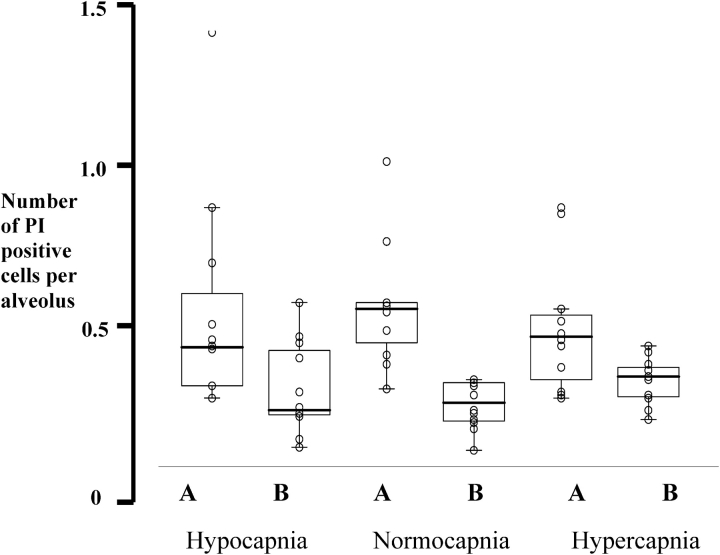
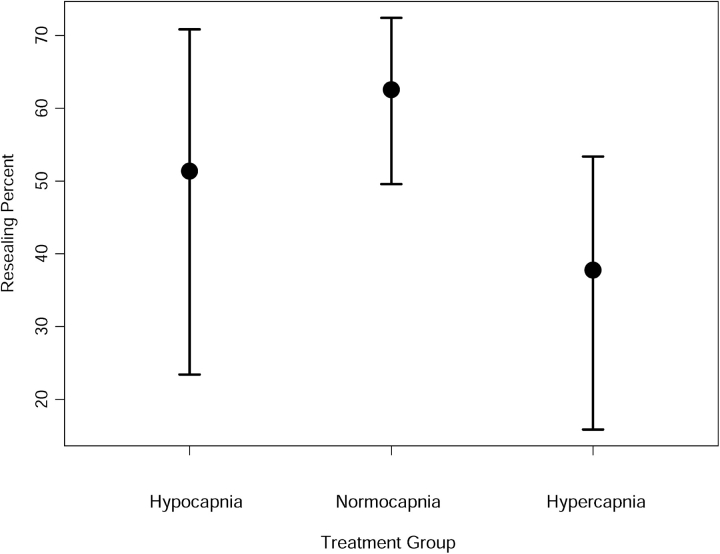
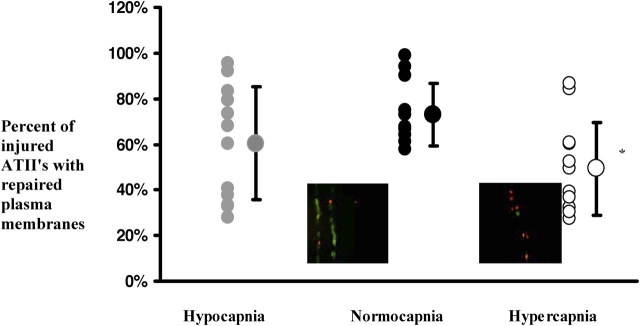
The objective of this study was to assess the effects of hypercapnic acidosis on lung cell injury and repair by confocal microscopy in a model of ventilator-induced lung injury. Three groups of normocapnic, hypocapnic, and hypercapnic rat lungs were perfused ex vivo, either during or after injurious ventilation, with a solution containing the membrane-impermeant label propidium iodide. In lungs labeled during injurious ventilation, propidium iodide fluorescence identifies all cells with plasma membrane wounds, both permanent and transient, whereas in lungs labeled after injurious ventilation propidium iodide fluorescence identifies only cells with permanent plasma membrane wounds. Hypercapnia minimized the adverse effects of high-volume ventilation on vascular barrier function, whereas hypocapnia had the opposite effect. Despite CO2-dependent differences in lung mechanics and edema the number of injured subpleural cells per alveolus was similar in the three groups (0.48 +/- 0.34 versus 0.51 +/- 0.19 versus 0.43 +/- 0.20 for hypocapnia, normocapnia, and hypercapnia, respectively). However, compared with normocapnia the probability of wound repair was significantly reduced in hypercapnic lungs (63 versus 38%; p < 0.02). This finding was subsequently confirmed in alveolar epithelial cell scratch models. The potential relevance of these observations for lung inflammation and remodeling after mechanical injury is discussed.
Figures
Similar articles
-
Impact of buffering hypercapnic acidosis on cell wounding in ventilator-injured rat lungs.Am J Physiol Lung Cell Mol Physiol. 2009 Jan;296(1):L140-4. doi: 10.1152/ajplung.90339.2008. Epub 2008 Nov 7. Am J Physiol Lung Cell Mol Physiol. 2009. PMID: 18996901 Free PMC article.
-
Ventilator-induced cell wounding and repair in the intact lung.Am J Respir Crit Care Med. 2003 Apr 15;167(8):1057-63. doi: 10.1164/rccm.200208-889OC. Epub 2002 Dec 12. Am J Respir Crit Care Med. 2003. PMID: 12480613
-
Hypercapnic acidosis attenuates ventilation-induced lung injury by a nuclear factor-κB-dependent mechanism.Crit Care Med. 2012 Sep;40(9):2622-30. doi: 10.1097/CCM.0b013e318258f8b4. Crit Care Med. 2012. PMID: 22732277
-
Effects of hypercapnia and hypercapnic acidosis on attenuation of ventilator-associated lung injury.Minerva Anestesiol. 2011 Jul;77(7):723-33. Minerva Anestesiol. 2011. PMID: 21709659 Review.
-
Carbon dioxide in the critically ill: too much or too little of a good thing?Respir Care. 2014 Oct;59(10):1597-605. doi: 10.4187/respcare.03405. Respir Care. 2014. PMID: 25261559 Review.
Cited by
-
Moderately high frequency ventilation with a conventional ventilator allows reduction of tidal volume without increasing mean airway pressure.Intensive Care Med Exp. 2014 Dec;2(1):13. doi: 10.1186/2197-425X-2-13. Epub 2014 May 9. Intensive Care Med Exp. 2014. PMID: 26266914 Free PMC article.
-
Mechanical ventilation guidelines in lung lobectomy surgery and the quest to improve outcomes.J Thorac Dis. 2018 Dec;10(12):6396-6398. doi: 10.21037/jtd.2018.11.52. J Thorac Dis. 2018. PMID: 30746173 Free PMC article. No abstract available.
-
Hypercapnia: a nonpermissive environment for the lung.Am J Respir Cell Mol Biol. 2012 Apr;46(4):417-21. doi: 10.1165/rcmb.2011-0395PS. Epub 2012 Jan 12. Am J Respir Cell Mol Biol. 2012. PMID: 22246860 Free PMC article. Review.
-
Sensing, physiological effects and molecular response to elevated CO2 levels in eukaryotes.J Cell Mol Med. 2009 Nov-Dec;13(11-12):4304-18. doi: 10.1111/j.1582-4934.2009.00952.x. Epub 2009 Oct 23. J Cell Mol Med. 2009. PMID: 19863692 Free PMC article. Review.
-
Very low tidal volume ventilation with associated hypercapnia--effects on lung injury in a model for acute respiratory distress syndrome.PLoS One. 2011;6(8):e23816. doi: 10.1371/journal.pone.0023816. Epub 2011 Aug 19. PLoS One. 2011. PMID: 21886825 Free PMC article.
References
-
- Tobin MJ. Medical progress: advances in mechanical ventilation. N Engl J Med 2001;344:1986–1996. - PubMed
-
- McConnell R, MacIntyre NR. Tracheal gas insufflation. Semin Respir Crit Care Med 2000;21:211–214. - PubMed
-
- Feihl F, Perret C. Permissive hypercapnia: how permissive should we be? Am J Respir Crit Care Med 1994;150:1722–1737. - PubMed
-
- Shibata K, Cregg N, Englelberts D, Takeuchi A, Fedorko L, Kavanagh BP. Hypercapnic acidosis may attenuate acute lung injury by inhibition of endogenous xanthine oxidase. Am J Respir Crit Care Med 1999;158:1578–1584. - PubMed
-
- Broccard AF. Protective effects of hypercapnic acidosis on ventilator-induced lung injury. Am J Respir Crit Care Med 2001;164:802–806. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
