

Review
doi: 10.1128/JCM.43.2.973-977.2005.
Scedosporium apiospermum soft tissue infection successfully treated with voriconazole: potential pitfalls in the transition from intravenous to oral therapy
Affiliations
- PMID: 15695722
- PMCID: PMC548045
- DOI: 10.1128/JCM.43.2.973-977.2005
Item in Clipboard
Review
Scedosporium apiospermum soft tissue infection successfully treated with voriconazole: potential pitfalls in the transition from intravenous to oral therapy
J Clin Microbiol.
2005 Feb.
Abstract
An immunocompromised patient with an invasive soft tissue infection due to Scedosporium apiospermum was successfully treated with voriconazole and surgical debridement. After transition from intravenous to oral therapy, successive adjustments of the oral dose were required to achieve complete resolution. For soft tissue infections due to molds characterized by thin, septate hyphae branching at acute angles, voriconazole should be considered a first-line antifungal agent. The potential usefulness of plasma voriconazole levels for guiding optimal therapy should be investigated.
Figures
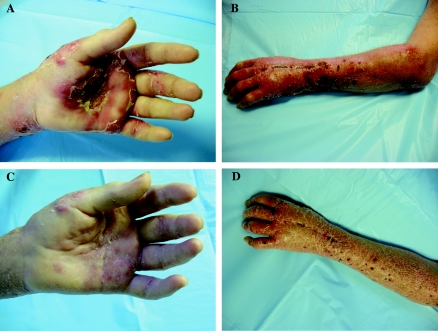
Left hand (A) and arm (B) of patient 1 week after transition from intravenous to oral voriconazole. The nodules and pustules form a pattern characteristic of lymphangitic spread. At 2 weeks after reinstitution of intravenous voriconazole therapy, the purulent nodules had disappeared from the hand (C) and arm (D).
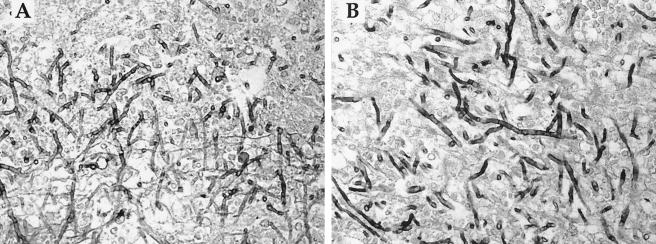
Histopathologic sections demonstrating the similarity between S. apiospermum (A) and A. fumigatus (B) in autopsy sections of cerebral tissues from immunosuppressed patients (Gomori-methenamine silver stain, ×600 magnification). Both fungi display thin, delicate, septate hyphae branching at acute angles. Note that these sections are provided for illustrative purposes and are not from the patient discussed in this case report.
Comment in
-
Molecular mycological diagnosis and correct antimycotic treatments.J Clin Microbiol. 2005 Jul;43(7):3584; author reply 3584-5. doi: 10.1128/JCM.43.7.3584-3585.2005. J Clin Microbiol. 2005. PMID: 16000516 Free PMC article. No abstract available.
Similar articles
-
Successful treatment of Scedosporium apiospermum soft tissue abscess with caspofungin and voriconazole in a severely immunocompromised patient with acute myeloid leukemia.Transpl Infect Dis. 2010 Dec;12(6):538-42. doi: 10.1111/j.1399-3062.2010.00537.x. Transpl Infect Dis. 2010. PMID: 20604906
-
Case of cutaneous Scedosporium apiospermum infection successfully treated with voriconazole.J Dermatol. 2009 Feb;36(2):98-102. doi: 10.1111/j.1346-8138.2009.00597.x. J Dermatol. 2009. PMID: 19284454
-
Successful outcome of Scedosporium apiospermum disseminated infection treated with voriconazole in a patient receiving corticosteroid therapy.Clin Infect Dis. 2000 Dec;31(6):1499-501. doi: 10.1086/317496. Clin Infect Dis. 2000. PMID: 11096022
-
Scedosporium apiospermum eumycetoma successfully treated with oral voriconazole: report of a case and review of the Brazilian reports on scedosporiosis.Rev Inst Med Trop Sao Paulo. 2013 Mar-Apr;55(2):121-3. doi: 10.1590/s0036-46652013000200010. Rev Inst Med Trop Sao Paulo. 2013. PMID: 23563766 Review.
-
Successful treatment of disseminated scedosporium infection in 2 lung transplant recipients: review of the literature and recommendations for management.J Heart Lung Transplant. 2006 Oct;25(10):1268-72. doi: 10.1016/j.healun.2006.06.002. J Heart Lung Transplant. 2006. PMID: 17045941 Review.
Cited by
-
Subcutaneous fungal infections.Curr Infect Dis Rep. 2012 Oct;14(5):530-9. doi: 10.1007/s11908-012-0275-3. Curr Infect Dis Rep. 2012. PMID: 22811027
-
A Case of Invasive Fungal Infection Due to Scedosporium apiospermum in a Patient with Psoriasis.Infect Drug Resist. 2023 Aug 8;16:5085-5090. doi: 10.2147/IDR.S420991. eCollection 2023. Infect Drug Resist. 2023. PMID: 37576520 Free PMC article.
-
Hand Mycetoma: The Mycetoma Research Centre Experience and Literature Review.PLoS Negl Trop Dis. 2016 Aug 2;10(8):e0004886. doi: 10.1371/journal.pntd.0004886. eCollection 2016 Aug. PLoS Negl Trop Dis. 2016. PMID: 27483367 Free PMC article. Review.
-
Scedosporiosis in a Combined Kidney and Liver Transplant Recipient: A Case Report of Possible Transmission from a Near-Drowning Donor.Case Rep Transplant. 2016;2016:1879529. doi: 10.1155/2016/1879529. Epub 2016 Dec 13. Case Rep Transplant. 2016. PMID: 28070441 Free PMC article.
-
Fungal rhinosinusitis caused by Scedosporium apiospermum in a cat.J Feline Med Surg. 2010 Dec;12(12):967-71. doi: 10.1016/j.jfms.2010.07.004. Epub 2010 Sep 17. J Feline Med Surg. 2010. PMID: 20851007 Free PMC article.
References
-
- Baden, L. R., J. T. Katz, J. A. Fishman, C. Koziol, A. DelVecchio, M. Doran, and R. H. Rubin. 2003. Salvage therapy with voriconazole for invasive fungal infections in patients failing or intolerant to standard antifungal therapy. Transplantation 76:1632-1637. - PubMed
-
- Barbaric, D., and P. J. Shaw. 2001. Scedosporium infection in immunocompromised patients: successful use of liposomal amphotericin B and itraconazole. Med. Pediatr. Oncol. 37:122-125. - PubMed
-
- Bosma, F., A. Voss, H. W. van Hamersvelt, R. G. de Sevaux, J. Biert, B. J. Kullberg, W. G. Melchers, and P. E. Verweij. 2003. Two cases of subcutaneous Scedosporium apiospermum infection treated with voriconazole. Clin. Microbiol. Infect. 9:750-753. - PubMed
-
- Canet, J. J., X. Pagerols, C. Sanchez, P. Vives, and J. Garau. 2001. Lymphocutaneous syndrome due to Scedosporium apiospermum. Clin. Microbiol. Infect. 7:648-650. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
