

Review
doi: 10.1371/journal.pmed.0020003.
Intermittent presumptive treatment for malaria
Affiliations
- PMID: 15696210
- PMCID: PMC545196
- DOI: 10.1371/journal.pmed.0020003
Item in Clipboard
Review
Intermittent presumptive treatment for malaria
PLoS Med.
2005 Jan.
Abstract
A better understanding of the pharmacodynamics of intermittent presumptive treatment, says White, will guide more rational policymaking
Conflict of interest statement
Figures
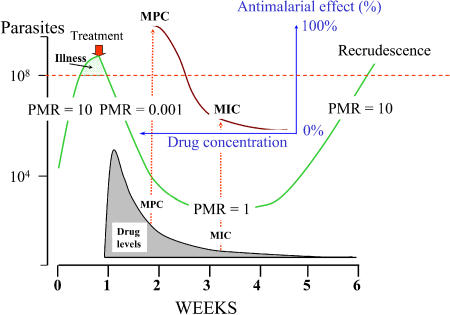
The parasite burden in an adult (vertical axis) is shown in green. After parasite burden expands to the point where it causes illness, treatment is given (red arrow), which causes a log-linear decline in parasite numbers until concentrations of the antimalarial drug (grey shading) fall below the MPC. As the antimalarial blood levels fall further, the decline in parasite burden slows until it reaches a multiplication rate of one (the antimalarial concentration at this point is the in vivo MIC). The parasite population then expands to cause a recrudescence six weeks later. The sigmoid concentration–effect relationship is shown in brown; it is depicted in the reverse direction to that normally drawn. PMR, parasite multiplication rate.
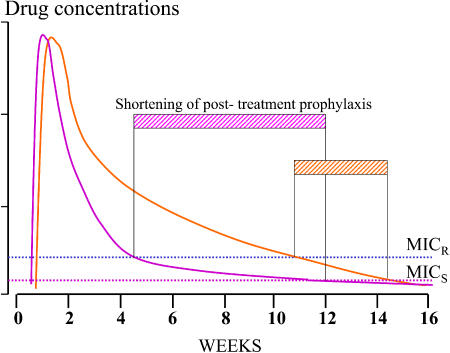
The examples shown here are mefloquine (orange) and chloroquine (pink). An increase in MIC has different effects on the shortening of post-treatment suppressive prophylaxis (hatched bars). MICR, MIC for resistant parasites; MICS, MIC for sensitive parasites.
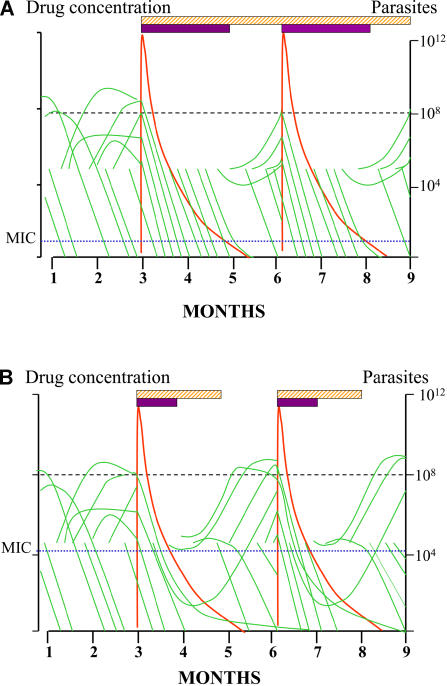
Entomological inoculation rate is about 50 infectious bites per person per year. Note that many infections self-cure (each infection is depicted as a green line). The hatched bars represent the duration of “suppressive prophylactic activity”, and the solid bars represent the period during which parasite multiplication is suppressed (i.e., levels exceed the in vivo MIC). The horizontal dotted line at 108 parasites represents the level at which malaria can be detected on a blood film. (A) represents a drug-sensitive area; (B) represents a moderately resistant area.
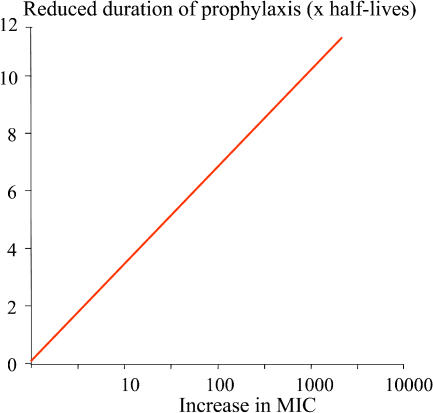
The proportional increase in malaria parasite MIC with resistance is plotted against the shortening of the duration of PTP, expressed as multiples of the terminal half-life. This applies only to drugs for which suppressive antimalarial prophylaxis occurs in the terminal elimination phase (i.e., most drugs).
Similar articles
-
Is chloroquine chemoprophylaxis still effective to prevent low birth weight? Results of a study in Benin.Malar J. 2007 Mar 6;6:27. doi: 10.1186/1475-2875-6-27. Malar J. 2007. PMID: 17341298 Free PMC article. Clinical Trial.
-
[Malaria in pregnancy: a therapeutic dilemma].Med Sci (Paris). 2009 Oct;25(10):867-9. doi: 10.1051/medsci/20092510867. Med Sci (Paris). 2009. PMID: 19849992 French. No abstract available.
-
[Resistance to sulfadoxine-pyrimethamine and pregnancy].Med Sante Trop. 2012 Oct-Dec;22(4):371. Med Sante Trop. 2012. PMID: 23610785 French. No abstract available.
-
Challenges in the concurrent management of malaria and HIV in pregnancy in sub-Saharan Africa.Lancet Infect Dis. 2006 Feb;6(2):100-11. doi: 10.1016/S1473-3099(06)70383-8. Lancet Infect Dis. 2006. PMID: 16439330 Review.
-
Current issues in the treatment of uncomplicated malaria in Africa.Br Med Bull. 2004 Dec 13;71:29-43. doi: 10.1093/bmb/ldh031. Print 2004. Br Med Bull. 2004. PMID: 15596867 Review.
Cited by
-
Quantifying Heterogeneous Malaria Exposure and Clinical Protection in a Cohort of Ugandan Children.J Infect Dis. 2016 Oct 1;214(7):1072-80. doi: 10.1093/infdis/jiw301. Epub 2016 Aug 1. J Infect Dis. 2016. PMID: 27481862 Free PMC article.
-
The impact of IPTi and IPTc interventions on malaria clinical burden - in silico perspectives.PLoS One. 2009 Aug 13;4(8):e6627. doi: 10.1371/journal.pone.0006627. PLoS One. 2009. PMID: 19675675 Free PMC article.
-
Intermittent preventive treatment for malaria in sub-saharan African: a halfway technology or a critical intervention?Am J Trop Med Hyg. 2010 May;82(5):755-6. doi: 10.4269/ajtmh.2010.825editorial. Am J Trop Med Hyg. 2010. PMID: 20439949 Free PMC article. No abstract available.
-
Implementation of intermittent preventive treatment in pregnancy with sulphadoxine/pyrimethamine (IPTp-SP) at a district health centre in rural Senegal.Malar J. 2008 Nov 7;7:234. doi: 10.1186/1475-2875-7-234. Malar J. 2008. PMID: 18992140 Free PMC article.
-
Prevention of malaria in pregnancy: The threat of sulfadoxine-pyrimethamine resistance.Front Pediatr. 2022 Aug 18;10:966402. doi: 10.3389/fped.2022.966402. eCollection 2022. Front Pediatr. 2022. PMID: 36061376 Free PMC article.
References
-
- Schultz LJ, Steketee RW, Macheso A, Kazembe P, Chitsulo L, et al. The efficacy of antimalarial regimens containing sulfadoxine-pyrimethamine and/or chloroquine in preventing peripheral and placental Plasmodium falciparum infection among pregnant women in Malawi. Am J Trop Med Hyg. 1994;51:515–522. - PubMed
-
- Verhoeff FH, Brabin BJ, Chimsuku L, Kazembe P, Russell WB, et al. An evaluation of the effects of intermittent sulfadoxine-pyrimethamine treatment in pregnancy on parasite clearance and risk of low birthweight in rural Malawi. Ann Trop Med Parasitol. 1998;92:141–150. - PubMed
-
- Parise ME, Ayisi JG, Nahlen BL, Schultz LJ, Roberts JM, et al. Efficacy of sulfadoxine-pyrimethamine for prevention of placental malaria in an area of Kenya with a high prevalence of malaria and human immunodeficiency virus infection. Am J Trop Med Hyg. 1998;59:813–822. - PubMed
-
- Shulman CE, Dorman EK, Cutts F, Kawuondo K, Bulmer JN, et al. Intermittent sulphadoxine-pyrimethamine to prevent severe anaemia secondary to malaria in pregnancy: A randomised placebo-controlled trial. Lancet. 1999;353:632–636. - PubMed
-
- Njagi JK, Magnussen P, Estambale B, Ouma J, Mugo B. Prevention of anaemia in pregnancy using insecticide-treated bednets and sulfadoxine-pyrimethamine in a highly malarious area of Kenya: A randomized controlled trial. Trans R Soc Trop Med Hyg. 2003;97:277–282. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
