

Introduction to alcohol withdrawal
- PMID: 15706727
- PMCID: PMC6761824
Introduction to alcohol withdrawal
Abstract
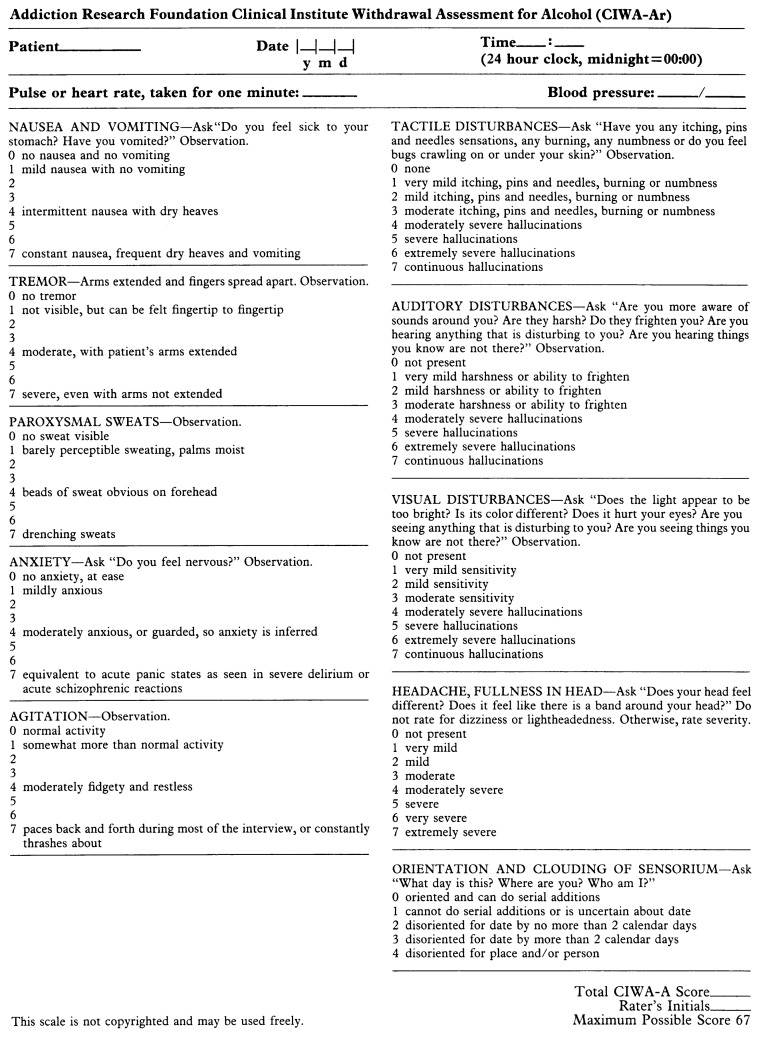
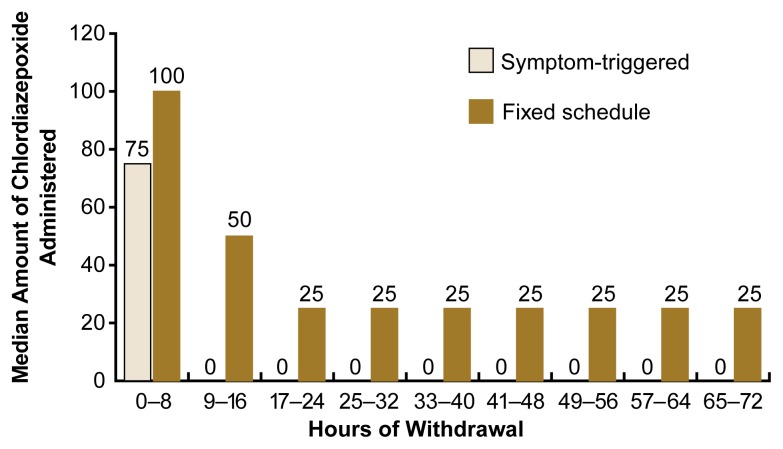
Heavy drinkers who suddenly decrease their alcohol consumption or abstain completely may experience alcohol withdrawal (AW). Signs and symptoms of AW can include, among others, mild to moderate tremors, irritability, anxiety, or agitation. The most severe manifestations of withdrawal include delirium tremens, hallucinations, and seizures. These manifestations result from alcohol-induced imbalances in the brain chemistry that cause excessive neuronal activity if the alcohol is withheld. Management of AW includes thorough assessment of the severity of the patient's symptoms and of any complicating conditions as well as treatment of the withdrawal symptoms with pharmacological and nonpharmacological approaches. Treatment can occur in both inpatient and outpatient settings. Recognition and treatment of withdrawal can represent a first step in the patient's recovery process.
Figures
Similar articles
-
Treatment of alcohol withdrawal.Alcohol Health Res World. 1998;22(1):38-43. Alcohol Health Res World. 1998. PMID: 15706731 Free PMC article. Review.
-
Outpatient management of alcohol withdrawal syndrome.Am Fam Physician. 2013 Nov 1;88(9):589-95. Am Fam Physician. 2013. PMID: 24364635 Review.
-
Complications of alcohol withdrawal: pathophysiological insights.Alcohol Health Res World. 1998;22(1):61-6. Alcohol Health Res World. 1998. PMID: 15706735 Free PMC article. Review.
-
Kindling in alcohol withdrawal.Alcohol Health Res World. 1998;22(1):25-33. Alcohol Health Res World. 1998. PMID: 15706729 Free PMC article. Review.
-
Alcohol withdrawal syndrome: how to predict, prevent, diagnose and treat it.Prescrire Int. 2007 Feb;16(87):24-31. Prescrire Int. 2007. PMID: 17323538
Cited by
-
Delirium Tremens: Assessment and Management.J Clin Exp Hepatol. 2018 Dec;8(4):460-470. doi: 10.1016/j.jceh.2018.04.012. Epub 2018 May 5. J Clin Exp Hepatol. 2018. PMID: 30564004 Free PMC article. Review.
-
Alcoholism treatment in the United States. An overview.Alcohol Res Health. 1999;23(2):69-77. Alcohol Res Health. 1999. PMID: 10890799 Free PMC article. Review.
-
Assessment of affective and somatic signs of ethanol withdrawal in C57BL/6J mice using a short-term ethanol treatment.Alcohol. 2015 May;49(3):237-43. doi: 10.1016/j.alcohol.2015.02.003. Epub 2015 Mar 6. Alcohol. 2015. PMID: 25817777 Free PMC article.
-
Involvement of delta opioid receptors in alcohol withdrawal-induced mechanical allodynia in male C57BL/6 mice.Drug Alcohol Depend. 2016 Oct 1;167:190-8. doi: 10.1016/j.drugalcdep.2016.08.017. Epub 2016 Aug 21. Drug Alcohol Depend. 2016. PMID: 27567436 Free PMC article.
-
Supplementing the liquid alcohol diet with chow enhances alcohol intake in C57 BL/6 mice.Drug Alcohol Depend. 2008 Sep 1;97(1-2):86-93. doi: 10.1016/j.drugalcdep.2008.03.022. Epub 2008 May 13. Drug Alcohol Depend. 2008. PMID: 18479843 Free PMC article.
References
-
- Begleiter H, Kissin B, editors. The Pharmacology of Alcohol and Alcohol Dependence. New York: Oxford University Press; 1996.
-
- Cutshall BJ. The Saunders-Sutton syndrome: An analysis of delirium tremens. Quarterly Journal of Studies on Alcohol. 1964;26:423–448. - PubMed
-
- Dupont RL, Gold MS. Withdrawal and reward: Implications for detoxification and relapse prevention. Psychiatric Annals. 1995;25(11):663–668.
-
- Fiellin DA, Samet JH, O’Connor PG. Reducing bias in observational research on alcohol withdrawal syndrome. Substance Abuse. 1998;19:23–31. - PubMed
-
- Foy A, March S, Drinkwater V. Use of an objective clinical scale in the assessment and management of alcohol withdrawal in a large general hospital. Alcoholism: Clinical and Experimental Research. 1988;12:360–364. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical