

Aneurysmal subarachnoid hemorrhage: management strategies and clinical outcomes in a regional neuroscience center
- PMID: 15709138
- PMCID: PMC7974084
Aneurysmal subarachnoid hemorrhage: management strategies and clinical outcomes in a regional neuroscience center
Abstract
Background and purpose: Aneurysmal subarachnoid hemorrhage (SAH) affects six to eight people per 100,000 annually, yet the optimum management of this condition remains controversial. Although the International Subarachnoid Aneurysm Trial (ISAT) explored this area, only 28% of patients from our center were randomized in that study. Our purpose was to evaluate the treatment and outcomes of patients not recruited into ISAT.
Methods: Procedural data, adverse events, additional procedures, and length of hospital stay were recorded for 122 patients who came to our center with aneurysmal SAH. Modified Rankin Scale (MRS) was assessed at 2 months and at 1 year by a postal questionnaire and telephone interview.
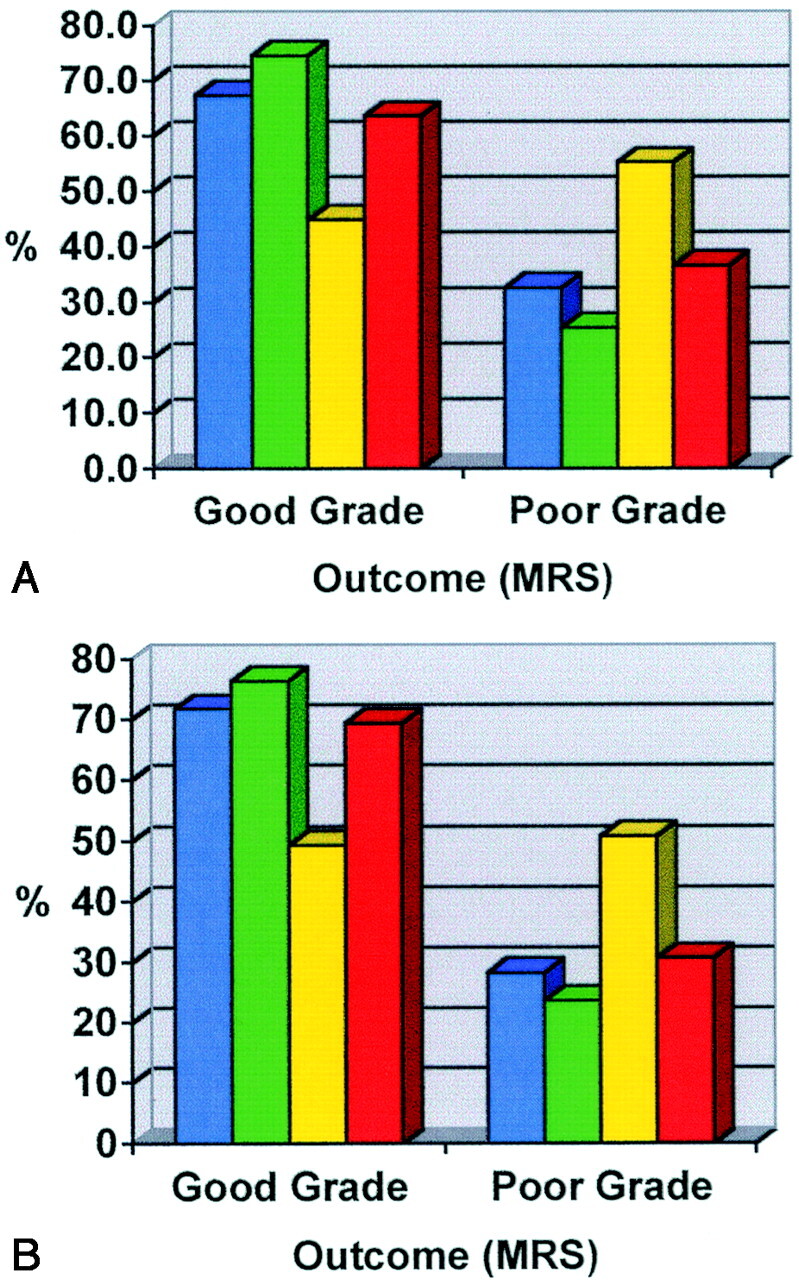
Results: Nine patients were treated conservatively, 67 underwent surgical clipping, and 46 underwent endovascular therapy. At 2 months, a good grade (MRS 0-2) was achieved in 67% of patients treated with endovascular therapy and in 45% of patients treated with surgery. At 1 year, a good grade was achieved in 72% in the endovascular group and 49% in the surgical group.
Conclusion: Endovascular therapy was a safe and effective treatment in a series of subjects who were not randomized in ISAT and in whom endovascular therapy was chosen over surgical clipping. The outcomes at 2 months and 1 year for those subjects treated with endovascular therapy were superior to the outcomes in those treated with surgical clipping. Our study was small and from a single center, but in this population the outcomes of endovascular treatment were similar to those reported by ISAT.
Figures
References
-
- Linn FH, Rinkel GJ, Algra A, van Gijn J. Incidence of subarachnoid hemorrhage: role of region, year, and rate of computed tomography—a meta-analysis. Stroke 1996;27:625–629 - PubMed
-
- Auer LM. Unfavorable outcome following early surgical repair of ruptured cerebral aneurysms: a critical review of 238 patients. Surg Neurol 1991;35:152–158 - PubMed
-
- Edner G, Kagstrom E, Wallstedt L. Total overall management and surgical outcome after aneurysmal subarachnoid hemorrhage in a defined population. Br J Neurosurg 1992;6:409–420 - PubMed
-
- Proust F, Hannequin D, Langlois O, Freger P, Creissard P. Causes of morbidity and mortality after ruptured aneurysm surgery in a series of 230 patients: the importance of control angiography. Stroke 1995;26:1553–1557 - PubMed
-
- Vinuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–482 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources