

Calprotectin is a stronger predictive marker of relapse in ulcerative colitis than in Crohn's disease
- PMID: 15710984
- PMCID: PMC1774401
- DOI: 10.1136/gut.2004.043406
Calprotectin is a stronger predictive marker of relapse in ulcerative colitis than in Crohn's disease
Abstract
Background and aims: The clinical course of inflammatory bowel disease is characterised by a succession of relapses and remissions. The aim of our study was to assess whether the predictive value of faecal calprotectin-a non-invasive marker of intestinal inflammation-for clinical relapse is different in ulcerative colitis (UC) and Crohn's disease (CD).
Methods: Seventy nine consecutive patients with a diagnosis of clinically quiescent inflammatory bowel disease (38 CD and 41 UC) were followed for 12 months, undergoing regular clinical evaluations and blood tests. A single stool sample was collected at the beginning of the study from each patient and the calprotectin concentration was assessed by a commercially available enzyme linked immunoassay.
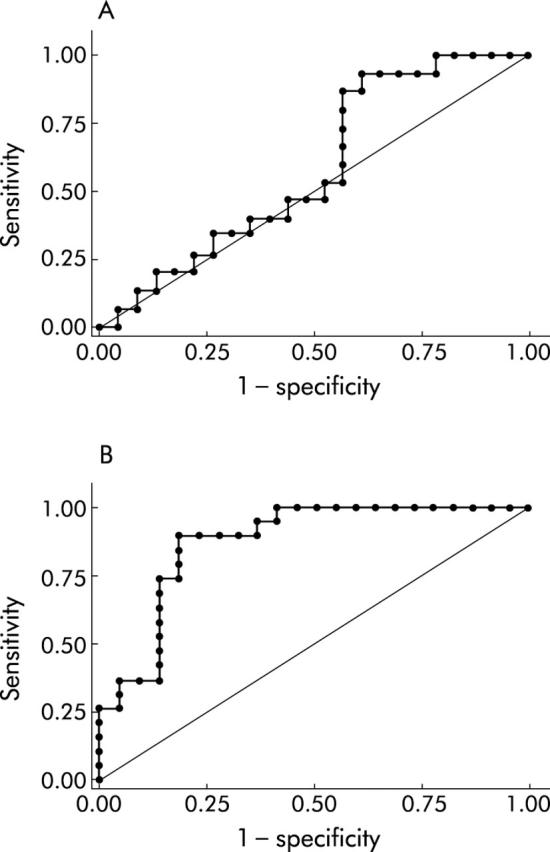
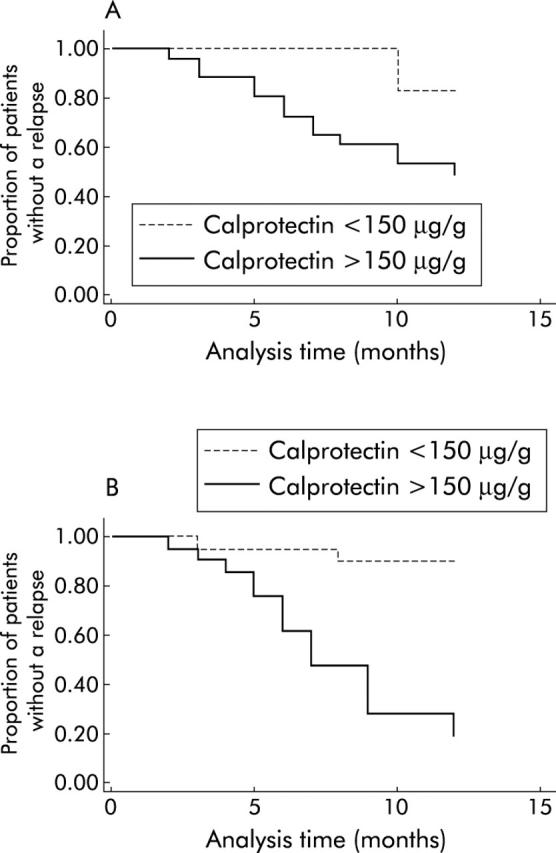
Results: In CD, median calprotectin values were 220.1 mug/g (95% confidence interval (CI) 21.7-418.5) in those patients who relapsed during follow up, and 220.5 mug/g (95% CI 53-388) in non-relapsing patients (p=0.395). In UC, median calprotectin values were 220.6 mug/g (95% CI 86-355.2) and 67 microg/g (95% CI 15-119) in relapsing and non-relapsing patients, respectively (p<0.0001). The multivariate Cox (proportional hazard) regression model, after adjustment for possible confounding variables, showed a twofold and 14-fold increase in the relapse risk, respectively, in those patients with CD and UC in clinical remission who had a faecal calprotectin concentration higher than 150 microg/g.
Conclusions: Faecal calprotectin proved to be an even stronger predictor of clinical relapse in UC than in CD, which makes the test a promising non-invasive tool for monitoring and optimising therapy.
Figures
Comment in
-
Predicting relapse in patients with inflammatory bowel disease: what is the role of biomarkers?Gut. 2005 Mar;54(3):321-2. doi: 10.1136/gut.2004.048850. Gut. 2005. PMID: 15710974 Free PMC article. Review. No abstract available.
-
Inflammatory biomarkers predict relapse in IBD.Gut. 2005 Sep;54(9):1346-7. doi: 10.1136/gut.2005.070615. Gut. 2005. PMID: 16099806 Free PMC article. No abstract available.
-
Calprotectin and IBD.Gut. 2005 Sep;54(9):1349-50; author reply 1350. doi: 10.1136/gut.2005.070656. Gut. 2005. PMID: 16099812 Free PMC article. No abstract available.
References
-
- Modigliani R, Mary JY, Simon JF, et al. Clinical, biological, and endoscopic picture of attacks of Crohn’s disease. Gastroenterology 1990;98:811–18. - PubMed
-
- Biancone L, De Nigris F, Del Vecchio Blanco G, et al. Review article: monitoring the activity of Crohn’s disease. Aliment Pharmacol Ther 2002;16 (suppl 4) :29–33. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical