

Review
doi: 10.1136/gut.2003.035907.
Management of acute pancreatitis: from surgery to interventional intensive care
Affiliations
- PMID: 15710995
- PMCID: PMC1774421
- DOI: 10.1136/gut.2003.035907
Item in Clipboard
Review
Management of acute pancreatitis: from surgery to interventional intensive care
Gut.
2005 Mar.
No abstract available
Figures
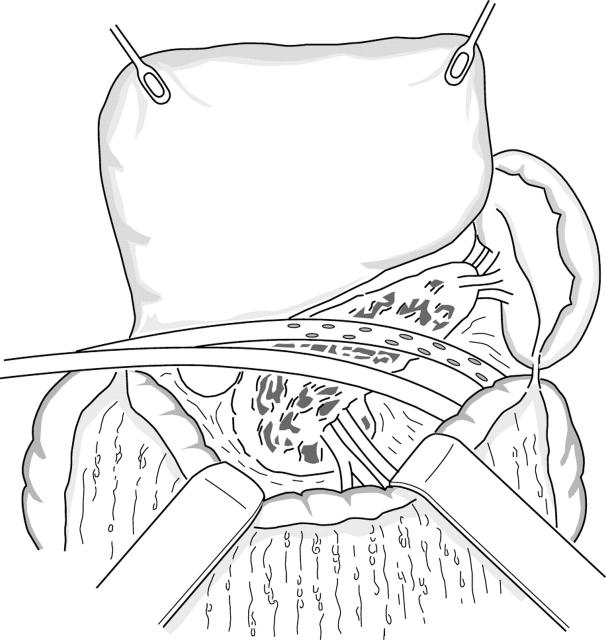
Closed lavage of the debrided cavity. The lesser sac is opened and the greater omentum divided close to the gastroepiploic vessels. Four catheters are inserted (two from each side) for postoperative continuous lavage of the lesser sac. The tip of the catheters are placed at the tail of the pancreas and behind the descending colon, as well as at the head of the gland and behind the ascending colon.

Closed lavage of the debrided cavity. The lesser sac is closed by suturing the greater omentum to the transverse colon for closed postoperative lavage.
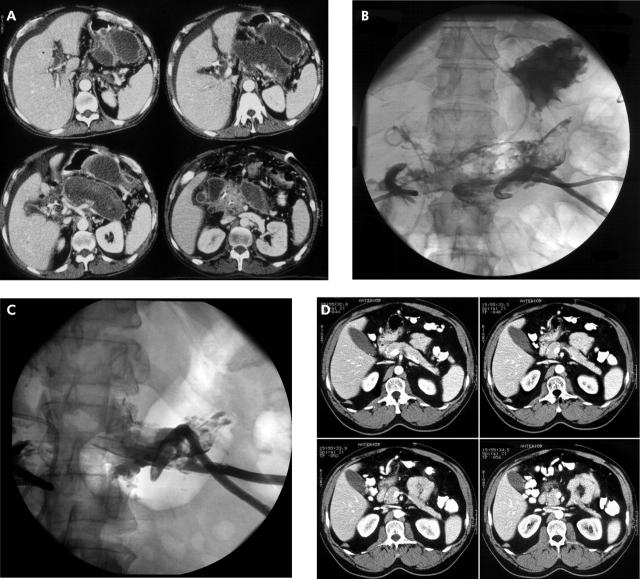
(A–D) Percutaneous necrosectomy in a 50 year old male with necrotising pancreatitis based on alcohol abuse. (A) Computed tomography (CT) scan before therapy revealed an acute necrotising pancreatitis showing typical findings such as peripancreatic fluid collections and pancreatic necrosis. (B) After CT guided placement of three 16 F catheters, contrast media was applied: filling defects represent solid necrotic tissue. In addition, there was a fistula between the necrotic cavity and the stomach, as indicated by contrast media within the stomach. (C) After percutaneous removal of necrotic tissue, the cavity decreased in size and demonstrated only a few small filling defects. (D) CT scan three years after necrosectomy: normal appearance of the pancreatic head. The pancreatic body and tail cannot be delineated, resulting in an anatomical situation such as after left sided surgical pancreatectomy.
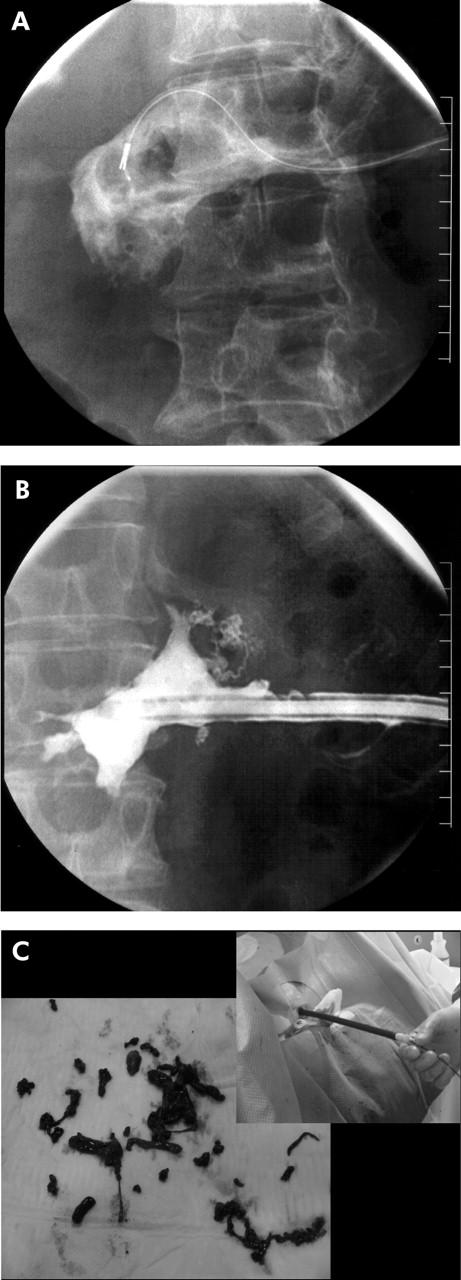
(A–C) Necrosis of the pancreatic body and tail: After installation of a 20 F peel away sheet, a snare catheter and a Dormia basket were inserted for necrosectomy (A). After necrosectomy, the necrotic cavity was reduced without any filling defects, which would represent residual necrosis (B). Macroscopic necrotic tissue was removed using the percutaneous technique of necrosectomy (C) described by Mann and colleagues.
References
-
- Isenmann R, Beger H. Natural history of acute pancreatoitis and the role of infection. Baillieres Best Pract Res Clin Gastroenterol 1999;13:291–301. - PubMed
-
- Klar E, Werner J. New pathophysiological findings in acute pancreatitis. Chirurgia 2000;71:253–64.
-
- Buter A, Imrie C, Carter C, et al. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. Br J Surg 2002;89:298–302. - PubMed
-
- Gloor B, Muller CA, Worni M, et al. Pancreatic infection in severe pancreatitis: The role of fungus and multiresistent organisms. Arch Surg 2001;36:592–6. - PubMed
-
- Dervenis C, Johnson CD, Bassi C, et al. Diagnosis, objective assessment of severity, and management of acute pancreatitis. Int J Pancreatol 1999;25:195–200. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical