

Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis and positron emission tomography study
- PMID: 15716852
- PMCID: PMC4347944
- DOI: 10.1038/sj.jcbfm.9600073
Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis and positron emission tomography study
Abstract
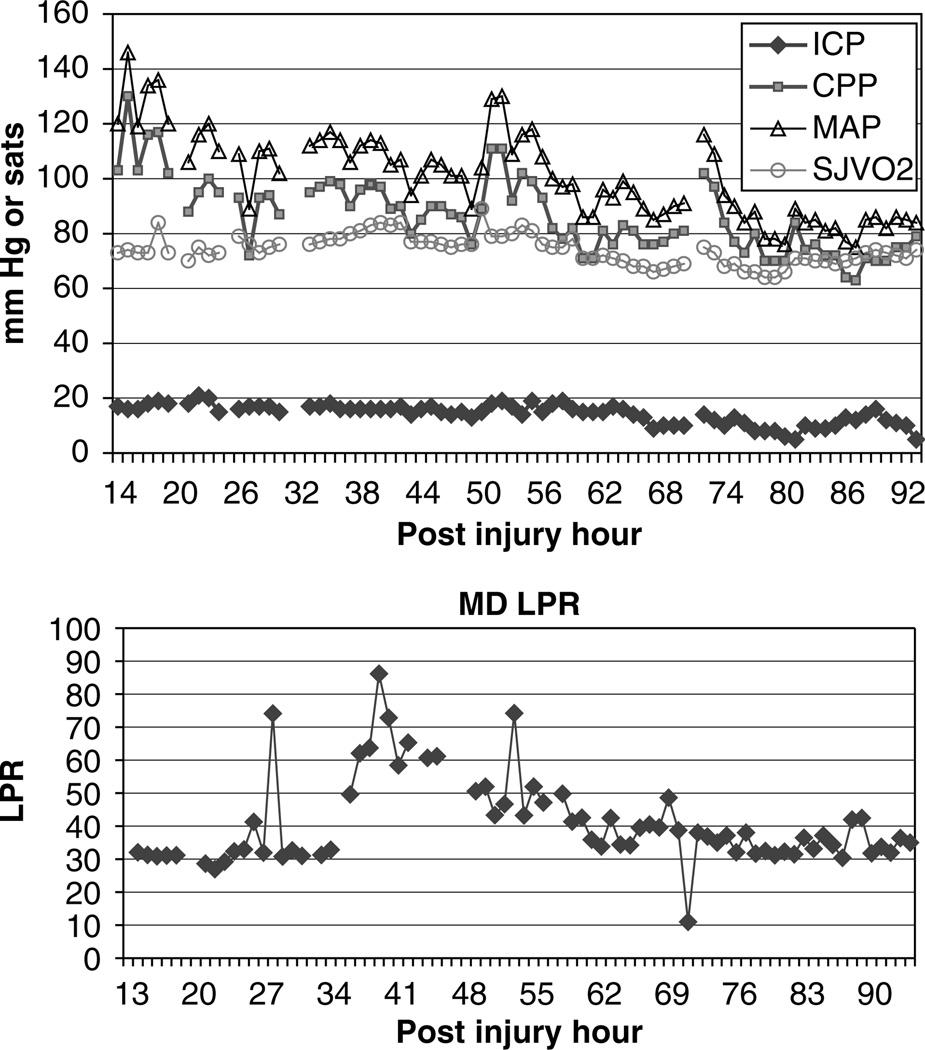
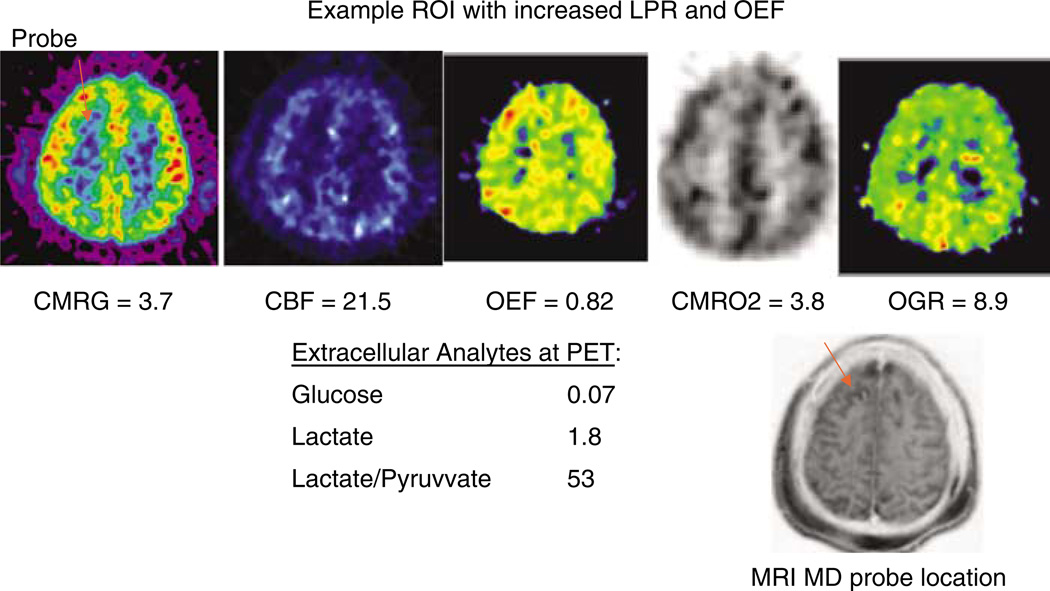
Brain trauma is accompanied by regional alterations of brain metabolism, reduction in metabolic rates and possible energy crisis. We hypothesize that microdialysis markers of energy crisis are present during the critical period of intensive care despite the absence of brain ischemia. In all, 19 brain injury patients (mean GCS 6) underwent combined positron emission tomography (PET) for metabolism of glucose (CMRglu) and oxygen (CMRO(2)) and cerebral microdialysis (MD) at a mean time of 36 h after injury. Microdialysis values were compared with the regional mean PET values adjacent to the probe. Longitudinal MD data revealed a 25% incidence rate of metabolic crisis (elevated lactate/pyruvate ratio (LPR) > 40) but only a 2.4% incidence rate of ischemia. Positron emission tomography imaging revealed a 1% incidence of ischemia across all voxels as measured by oxygen extraction fraction (OEF) and cerebral venous oxygen content (CvO(2)). In the region of the MD probe, PET imaging revealed ischemia in a single patient despite increased LPR in other patients. Lactate/pyruvate ratio correlated negatively with CMRO(2) (P < 0.001), but not with OEF or CvO(2). Traumatic brain injury leads to a state of persistent metabolic crisis as reflected by abnormal cerebral microdialysis LPR that is not related to ischemia.
Figures


References
-
- Ackerman RH, Lev MH, Mackay BC, Katz PM, Babikian VL, Alpert NM. PET studies in acute stroke findings and relevance to therapy (abstract) J Cereb Blood Flow Metab. 1989;9(S1):S359.
-
- Andersen BJ, Maramarou A. Isolated stimulation of glycolysis following traumatic brain injury. In: Hoff JT, Betz AL, editors. Intracranial pressure VII. Berlin: Springer; 1989. pp. 575–580.
-
- Baker SP, O’Neill B, Haddon W, Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187–196. - PubMed
-
- Bergsneider MA, Hovda DA, Shalmon E, Kelly DF, Vespa PM, Martin NA, Phelps ME, McArthur DL, Caron MJ, Kraus JF, Becker DP. Cerebral hyperglycolysis following severe human traumatic brain injury: a positron emission tomography study. J Neurosurg. 1997;86:241–251. - PubMed
-
- Bergsneider M, Hovda DA, Lee SM, Kelly DF, McArthur DL, Vespa PM, Lee JH, Huang SC, Martin NA, Phelps ME, Becker DP. Dissociation of cerebral glucose metabolism and level of consciousness during the period of metabolic depression following human traumatic brain injury. J Neurotrauma. 2000;17:389–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
