

Biomarkers and surrogate outcomes in neurodegenerative disease: lessons from multiple sclerosis
- PMID: 15717029
- PMCID: PMC534945
- DOI: 10.1602/neurorx.1.2.284
Biomarkers and surrogate outcomes in neurodegenerative disease: lessons from multiple sclerosis
Abstract
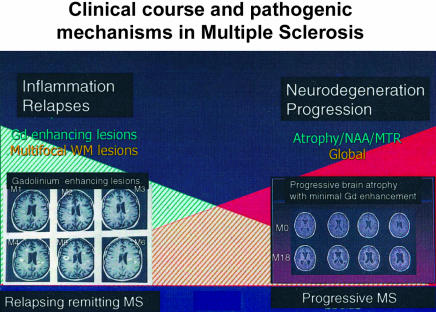
Multiple sclerosis (MS) is a chronic disease of the CNS that most commonly affects young adults. It is usually characterized in the early years by acute relapses followed by partial or complete remission; in later years progressive and irreversible disability develops. Because of the protracted and unpredictable clinical course, biological surrogate markers are much needed to make clinical trials of potential disease-modifying treatments more efficient. Magnetic resonance (MR) outcome measures are now widely used to monitor treatment outcome in MS trials. Areas of multifocal inflammation are detected with a high sensitivity as new areas of gadolinium enhancement and T2 abnormality, and these may be considered as surrogate markers for clinical relapses. However, progressive disability is not clearly related to inflammatory lesions but rather to a progressive and diffuse process with increasing neuroaxonal loss. MR surrogate measures for neuroaxonal loss include atrophy (tissue loss in brain and spinal cord), N-acetyl aspartate, and T1 hypointense lesions. Diffuse abnormality in normal appearing brain tissue may also be monitored using magnetization transfer ratio and other quantitative MR measures. For treatment trials of new agents aimed at preventing disability, measures of neuroaxonal damage should be acquired, especially atrophy, which occurs at all stages of MS and which can be quantified in a sensitive and reproducible manner. Because the MR surrogates for neuroaxonal loss are not yet validated as predicting future disability, definitive trials should continue to monitor an appropriate disability endpoint.
Figures
References
-
- Trapp BD, Peterson J, Ransohoff RM, Rudick R, Mork S, Bo L. Axonal transection in the lesions of multiple sclerosis. N Engl J Med 338: 278–285, 1998. - PubMed
-
- Lassmann H, Suchanek G, Ozawa K. Histopathology and the blood-cerebrospinal fluid barrier in multiple sclerosis. Ann Neurol 36(Suppl): S42–S46, 1994. - PubMed
-
- Thompson A, Kermode A, MacManus D, Kendall B, Kingsley D, Moseley I, McDonald W. Major differences in the dynamics of primary and secondary progressive multiple sclerosis. Ann Neurol 29: 53–62, 1991. - PubMed
-
- Allen IV, McKeown SR. A histological, histochemical and biochemical study of the macroscopically normal white matter in multiple sclerosis. J Neurol Sci 41: 81–89, 1979. - PubMed
-
- Evangelou N, Esiri MM, Smith S, Palace J, Mathews PM. Quantitative pathological evidence for axonal loss in normal appearing white matter in multiple sclerosis. Ann Neurol 47: 391–395, 2000. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
