

Fructose, insulin resistance, and metabolic dyslipidemia
- PMID: 15723702
- PMCID: PMC552336
- DOI: 10.1186/1743-7075-2-5
Fructose, insulin resistance, and metabolic dyslipidemia
Abstract
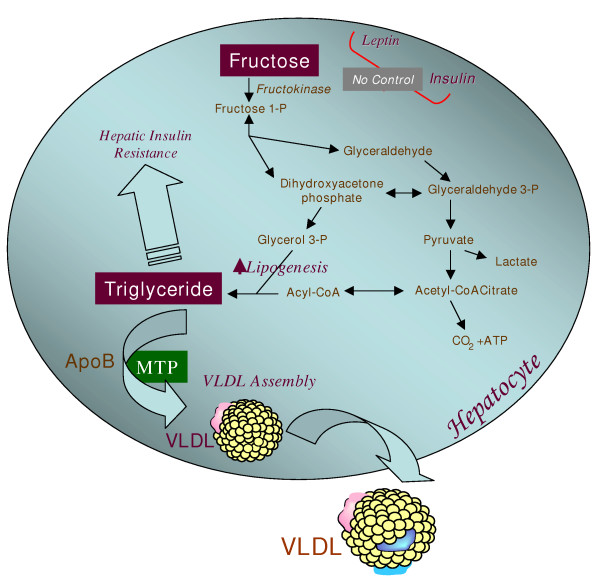
Obesity and type 2 diabetes are occurring at epidemic rates in the United States and many parts of the world. The "obesity epidemic" appears to have emerged largely from changes in our diet and reduced physical activity. An important but not well-appreciated dietary change has been the substantial increase in the amount of dietary fructose consumption from high intake of sucrose and high fructose corn syrup, a common sweetener used in the food industry. A high flux of fructose to the liver, the main organ capable of metabolizing this simple carbohydrate, perturbs glucose metabolism and glucose uptake pathways, and leads to a significantly enhanced rate of de novo lipogenesis and triglyceride (TG) synthesis, driven by the high flux of glycerol and acyl portions of TG molecules from fructose catabolism. These metabolic disturbances appear to underlie the induction of insulin resistance commonly observed with high fructose feeding in both humans and animal models. Fructose-induced insulin resistant states are commonly characterized by a profound metabolic dyslipidemia, which appears to result from hepatic and intestinal overproduction of atherogenic lipoprotein particles. Thus, emerging evidence from recent epidemiological and biochemical studies clearly suggests that the high dietary intake of fructose has rapidly become an important causative factor in the development of the metabolic syndrome. There is an urgent need for increased public awareness of the risks associated with high fructose consumption and greater efforts should be made to curb the supplementation of packaged foods with high fructose additives. The present review will discuss the trends in fructose consumption, the metabolic consequences of increased fructose intake, and the molecular mechanisms leading to fructose-induced lipogenesis, insulin resistance and metabolic dyslipidemia.
Figures
References
-
- Astrup A, Finer N. Redefining type 2 diabetes: 'diabesity' or 'obesity dependent diabetes mellitus'? Obes Rev. 2000;1:57–59. - PubMed
-
- Mokdad AH, Ford ES, Bowman BA, Nelson DE, Engelgau MM, Vinicor F, Marks JS. Diabetes trends in the US: 1990–1998. Diabetes Care. 2000;23:1278–1283. - PubMed
-
- Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. Jama. 2001;286:1195–1200. - PubMed
-
- Mokdad AH, Serdula MK, Dietz WH, Bowman BA, Marks JS, Koplan JP. The spread of the obesity epidemic in the United States, 1991–1998. Jama. 1999;282:1519–1522. - PubMed
-
- Pan XR, Yang WY, Li GW, Liu J. Prevalence of diabetes and its risk factors in China, 1994. National Diabetes Prevention and Control Cooperative Group. Diabetes Care. 1997;20:1664–1669. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
